Drs. Matthew Palazzolo, Kimberly Petkovich Vaglio, Stephen Clark, and Jennifer Osborne Rudy, MA, RDH, University of Louisville School of Dentistry
 Abstract
Abstract
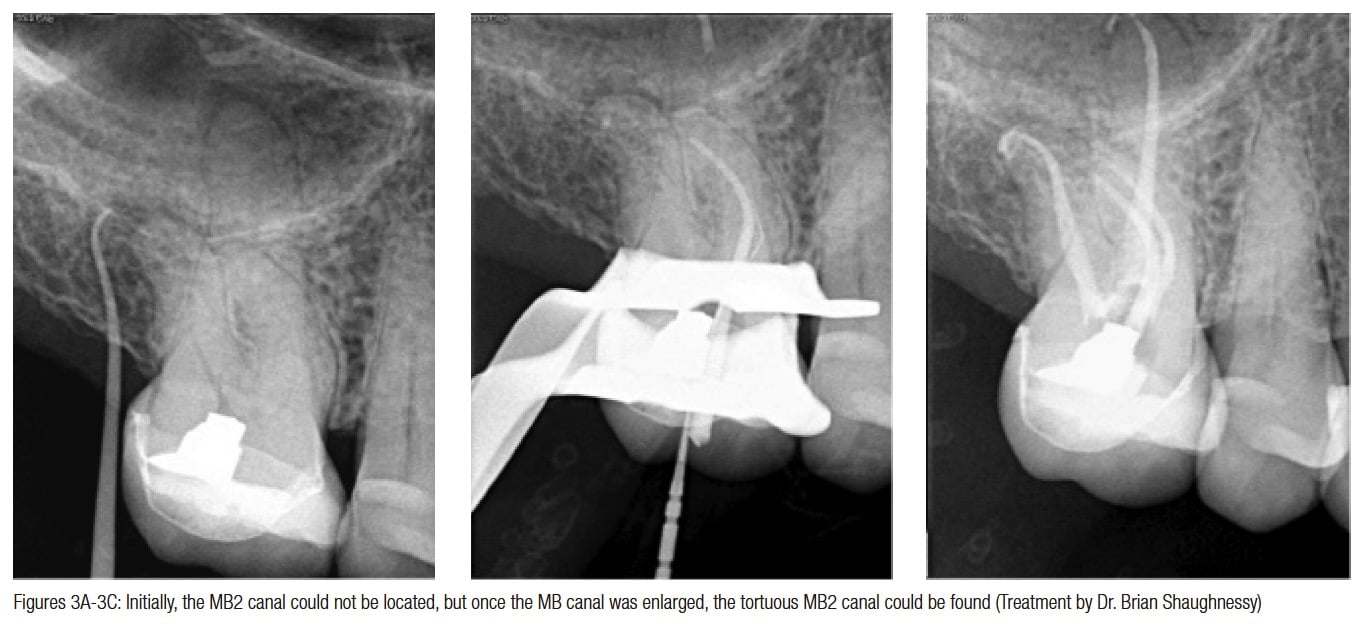
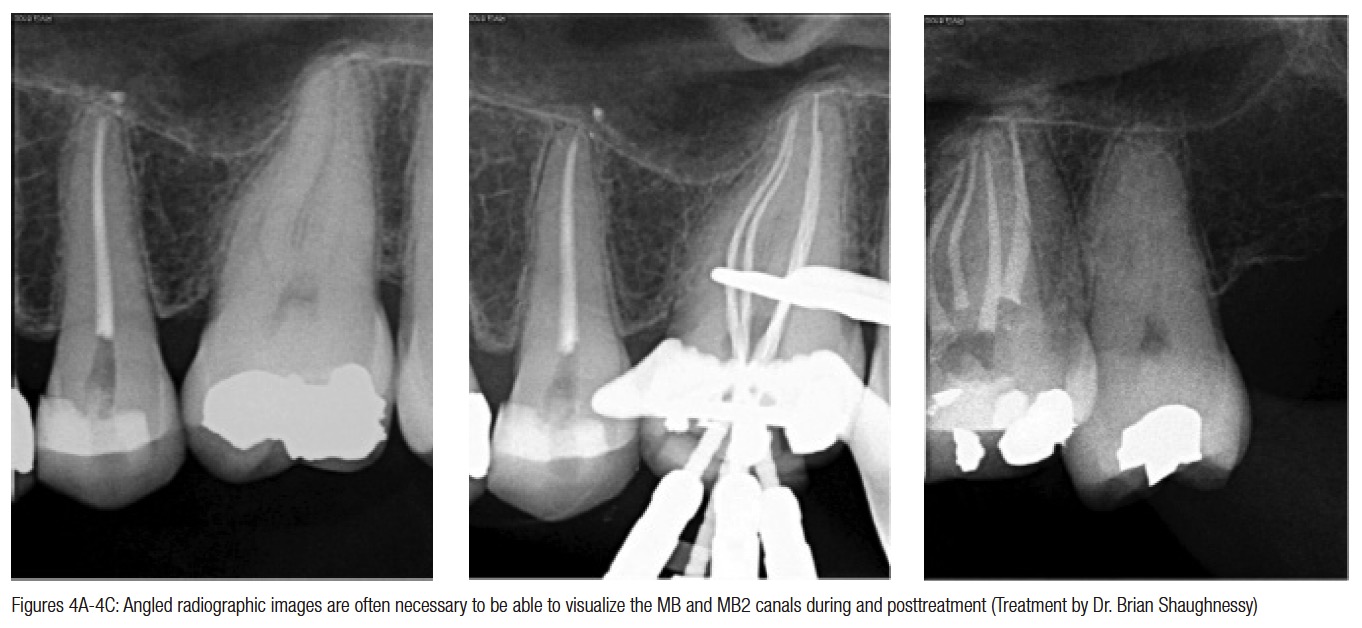
Background: The presence of a second canal in the mesiobuccal root (MB2) of maxillary molars is well documented in the literature. The purpose of this retrospective study was to assess the frequency of location of the MB2 canal in maxillary molars and variables affecting MB2 location by endodontic residents in a postgraduate endodontic program.
[userloggedin]
Methods: Electronic records and digital radiographs of patients treated in the post-graduate endodontic clinic between July 1, 2006, and June 30, 2013, were reviewed by two calibrated observers. Data collected included treating resident code, 1st-year/2nd-year resident, tooth number, patient age and gender, presence of preoperative crown, pulp vitality status, MB2 canal located (yes/no), initial treatment, or retreatment. MB2 was considered present if location was confirmed in the patient record and treatment radiographs. Pearson chi-square and one-way ANOVA were used for statistical analysis.
Results: 1,929 maxillary molars treated by 18 endodontic residents were reviewed. Frequency of locating the MB2 was 57.6% and ranged from 29.2%-71.8% among residents. Frequency of location of the MB2 was significantly greater by 2nd-year residents, with MB2 location by 51.9% of 1st-year residents compared to 61.9% by 2nd-year residents (p < 0.0001). Frequency of MB2 location was significantly lower in teeth with preoperative crowns (50.6% crown compared to 58.6% no crown (p < 0.05), while MB2 canal location was significantly higher in male patients (66.2%) than females (51.8%),
p < 0.0001.
Conclusion: Resident clinical experience was associated with frequency of location of the MB2 canal. Preoperative crowns were associated with increased difficulty locating the MB2 canal. The MB2 canal was found significantly more often in males than females.
 Background
Background
The successful outcome of nonsurgical root canal therapy is highly dependent upon location, thorough debridement, irrigation, and obturation of all canals and final restoration. Several studies have attempted to determine the presence of a second mesiobuccal canal (MB2) in maxillary molars.
Historically, roots were sectioned with magnification in order to determine the presence or absence of MB2. Using this methodology, Weine, et al.,1 found the MB2 canal in 52% of maxillary molars.
Kulild and Peters2 used a standard access and hand instruments to find the MB2 canal in 54% of 32 maxillary molars, then used long-shank endodontic round burs in the “subpulpal groove” to locate the MB2 in an additional 31%, and finally used a dental operating microscope after crown removal to locate the MB2 in another 10% for a total of 95% of their sample presenting with an MB2. Their results indicated that the presence of MB2 is high under ideal in vitro conditions and use of a microscope.
Some studies have also evaluated frequency of location of the MB2 canal in maxillary molars during clinical treatment. A clinical study conducted by Fogel, et al.,5 found the MB2 to be present in 71.2% of maxillary first molars. They attributed the higher number of clinically located MB2 canals to magnification, use of headlamps, and modified access preparations.
Stropko3 reported finding the MB2 canal in 93% of maxillary first molars and 60% of maxillary second molars after he became more experienced, used the dental operating microscope, allowed sufficient time for canal location, and used instruments adapted for micro-endodontics.
Using strict defined criteria for location of the MB2, Wolcott, et al.,6 found in a 5- year clinical investigation that the MB2 was located by six endodontists in 66% of first molars during retreatment, and 58% during initial treatment and in 40% of retreatments and 34% during initial treatment in second molars. The authors suggested that failure to find and treat existing MB2 canals can decrease the long-term prognosis.
Studies have also been done on MB2 location in postgraduate endodontic programs. Hartwell, et al.,7 reported that, within a postgraduate endodontic program, the MB2 was found in approximately 70% of 121 maxillary first molars.
Corcoran, et al.,8 reviewed MB2 location in clinical cases by three endodontic residents during their first 6 months of training and again during their last 6 months. The junior residents located the MB2 canal in 37% of 78 first molars and 46% of 37 second molars, while senior residents located the MB2 in 62% of 82 first molars and 63% of 40 second molars. The authors concluded that operator experience plays a significant role in the location and treatment of the MB2 canal.
A review of the above literature indicates that location of the MB2 canal varies greatly among practicing endodontists and endodontic residents.
 The purpose of this retrospective clinical study was to assess the frequency of location of the MB2 canal by endodontic residents in maxillary molars and evaluate variables affecting location frequency in a post-graduate endodontic program over a 6-year period.
The purpose of this retrospective clinical study was to assess the frequency of location of the MB2 canal by endodontic residents in maxillary molars and evaluate variables affecting location frequency in a post-graduate endodontic program over a 6-year period.
 Materials and methods
Materials and methods
This study reviewed the electronic records and digital radiographs of patients treated by 18 endodontic residents who received nonsurgical root canal therapy in the graduate endodontic program at the University of Louisville from July 1, 2006, through June 30, 2013. Radiographs and records were reviewed collaboratively by two endodontic residents. Data collected included treating resident code, 1st- or 2nd-year treating resident, tooth number, patient age and gender, presence of pre-operative crown, treated tooth pulp vitality status, MB2 located/not located, and initial treatment or retreatment.
The location of the MB2 in the patient record was verified by both endodontic residents collecting data. MB2 was considered to be present if:
- any portion of the MB2 could be visually observed in a postoperative or treatment radiograph with file or filling material present in the canal
- documentation was present for location of the MB2 in the patient record
All treating residents used a Global Operating Microscope (Global, St. Louis, Missouri) and were equipped with ultrasonics and various hand and rotary files. Chi-square analysis, odds ratio, and one-way ANOVA with Tukey’s post hoc analysis were used for statistical analysis. Data was recorded in SPSS version 22.
Results
The frequency of location of the MB2 canal in 1929 maxillary first and second molars was 57.6%. Among individual residents, the frequency of location by each resident varied widely from 29.2% to 71.8%.
Frequency of MB2 location increased from 51.9% during the 1st year of residency, to 61.9% during the 2nd year (Table 1).
The MB2 was found significantly more often in maxillary first molars at 64.2% (n = 904/1409) compared to maxillary second molars at 39.8% (n = 207/520) (Table 2).
When comparing gender, the MB2 was found more often in males at 66.2% (n = 516/780) compared to females at 51.8% (n = 595/1149) (Table 3).
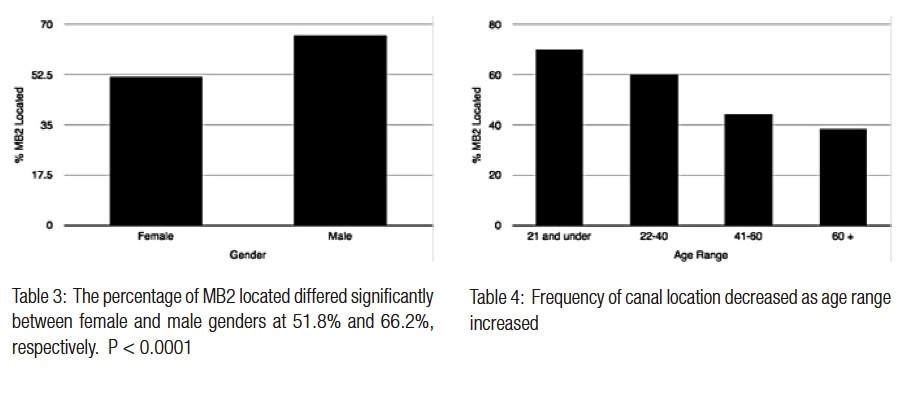
 The MB2 was found more frequently in younger patients. MB2 location ranged from a high of 70.1% in patients aged 21 and under to a low of 38.6% in patients aged 61 and older (Table 4). Significant differences were found between each age group with the exception of the comparison between age groups 41-60 and 60-plus (Table 5).
The MB2 was found more frequently in younger patients. MB2 location ranged from a high of 70.1% in patients aged 21 and under to a low of 38.6% in patients aged 61 and older (Table 4). Significant differences were found between each age group with the exception of the comparison between age groups 41-60 and 60-plus (Table 5).
Presence of a preoperative crown affected the frequency of location of the MB2. In teeth with a preoperative crown, the MB2 was located in 50.6% (n = 119/235), and in teeth without a crown, location frequency was 58.6% (n = 992/1694) (Table 6).

Discussion
The results of this retrospective study are similar to that of Corcoran, et al., in that greater resident experience was correlated with increased frequency of location of the MB2. While this study evaluated treatment on over 1,900 teeth, the study by Corcoran, et al., evaluated 100 teeth; however, the results were similar.
In the 5-year clinical investigation by Wolcott, et al.,5 the frequency of location of MB2 was very similar to this study. They located the MB2 in 60% of maxillary first molars and 35% of second molars. This study reported 64.2% in first molars and 39.8% in second molars. However, Wolcott, et al., used a stricter definition of MB2 location. Their numbers may have been even higher with the definition used in this study.

In this study, a significant difference was found in frequency of MB2 location between males (66.2%) and females (51.8%). These results agree with those of Fogel, et al.,3 and contrast with those of Neaverth, et al.,8 who found no difference by patient gender. Certainly, this is an interesting finding and should be pursued with further research on effects of patient gender and frequency of canal location.
This study reported that the MB2 was located more often in younger age groups. That finding has been reported previously by Fogel, et al.,3 Neaverth, et al.,8 and Gilles and Reader.9 One can speculate that increased pulpal calcification due to aging or extensive restoration leads to increased difficulty in locating the MB2 canal during the endodontic treatment.
 In this study, the MB2 was located less frequently in teeth with a preoperative crown. This finding could also be due to pulpal calcification and the loss of anatomic landmarks.
In this study, the MB2 was located less frequently in teeth with a preoperative crown. This finding could also be due to pulpal calcification and the loss of anatomic landmarks.
The results of this study indicate that location and subsequent clinical treatment of the MB2 canal is affected by multiple variables. Future research should be directed toward techniques/strategies to mitigate the effect of these variables on location/treatment of the MB2 canal.
The results of this study also indicate that in a teaching institution, endodontic faculty need to strive to make an additional effort to assist residents who are early in their training program in locating the MB2 canal during treatment of maxillary molars. Ideally, with faculty assistance, previous resident experience should not affect the frequency of MB2 canal location in a postgraduate endodontic program.
Conclusion
In this study, the MB2 canal was located significantly more often in maxillary first molars, males, younger patients, and teeth without a crown. The MB2 canal was also located significantly more frequently by residents in their 2nd year of training.
References
1. Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28(3):419-425. 2. Kulid JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod. 1990;16(7):311-317. 3. Fogel HM, Peikoff MD, Christie WH. Canal configuration in the mesiobuccal root of the maxillary first molar: a clinical study. J Endod. 1994;20(3):135-137. 4. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod. 1999;25(6):446-450. 5. Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S, Meyers J. A 5 yr clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. J Endod. 2005;31(4):262-264. 6. Hartwell G, Appelstein CM, Lyons WW, Guzek ME. The incidence of four canals in maxillary first molars: a clinical determination. J Am Dent Assoc. 2007;138(10):1344-1346. 7. Corcoran J, Apicella MJ, Mines P. The effect of operator experience in locating additional canals in maxillary molars. J Endod. 2007;33(1):15-17. 8. Neaverth EJ, Kotler LM, Kaltenbach RF. Clinical investigation (in vivo) of endodontically treated maxillary first molars. J Endod. 1987;13(10):506-512. 9. Gilles J, Reader A. An SEM investigation of the mesiolingual canal in human maxillary first and second molars. Oral Surg Oral Med Oral Pathol. 1990;70(5):638-643.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
