Drs. Nicola Maria Grande, Gianluca Plotino, Hany Mohamed Aly Ahmed, Stephen Cohen, and Frédéric Bukiet provide a clinical perspective on the reciprocating movement in endodontics
Shaping the root canal facilitates cleaning the root canal system (RCS) and is probably the most important phase in endodontic treatment. It includes the removal of pulp tissue, microorganisms, infected dentin, and root canal filling materials (RCFMs) in nonsurgical retreatments (Hülsmann, Peter, Dummer, 2005). Shaping the canal enhances the efficiency of irrigants and medicaments, and optimizes subsequent filling procedures (Hülsmann, Peter, Dummer, 2005; Frank, 1967).
In the last 2 decades, numerous advances in endodontic instrumentation have been developed to achieve proper enlargement of the main canal without procedural errors (Frank, 1967). Reciprocating motion (RM) had been extensively used with stainless steel (SS) files initially in the development of mechanical instrumentation in endodontics. RM applied to nickel-titanium files has many differences from the one used with SS (Grande, et al., 2015). RM has been a recent innovation employing nickel-titanium instrumentation systems that claim to better resist instrument separation, thus permitting easier treatment and thereby shortening the learning curve for nickel-titanium file systems.
Evolution of RM in endodontics — historical perspective
The early era of mechanical instrumentation
Automated instrumentation of the root canal space was an early objective of clinical endodontics, beginning in the 20th century, when pioneers were trying to develop mechanical instruments (Hülsmann, Peter, Dummer, 2005).
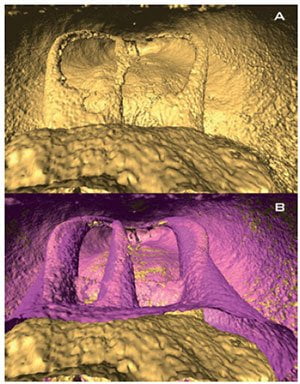
post-instrumentation three-dimensional reconstructions (in pink postoperative) showing the centering ability of the reciprocating technique
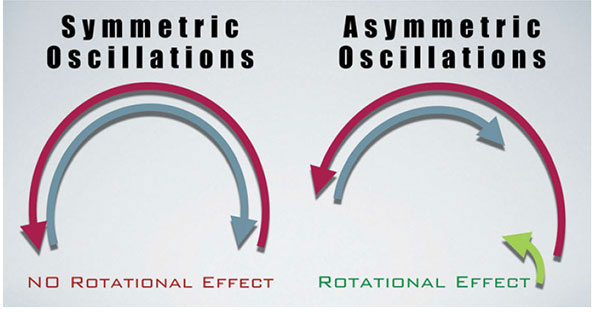
Rotary SS root canal instruments, such as Gates Glidden burs and Peeso reamers, can be safely used in the coronal, and sometimes the middle third of relatively straight RCS, but their stiffness increases the risk of root perforation as the clinician approaches the middle third of the canal (Laws, 1968; Jungmann, Uchin, Bucher, 1975; Martin, 1976). For this reason, a RM that has equal angles in both directions was successfully introduced. This type of symmetric reciprocation can be defined as complete oscillating reciprocation (Figure 1), resembling the classic watch-winding movement used with manual SS files.
In the 1960s, different handpieces were manufactured initially and designed to reciprocate at 90º (Frank, 1967). The overall results regarding the shaping ability and its safety were generally similar (Frank, 1967; Luebke, Brantley, 1990; Lausten, Luebke, Brantley, 1993) or inferior (Dihn, 1972; Molven, 1970; O’Connell, Brayton, 1975; Klayman, Brilliant, 1974; Sargenti, 1974; Weine, Kelly, Lio, 1975; Weine, Kelly, Bray, 1976; Powell, Simon, Maze, 1986) to a classic approach using SS manual root canal preparation (RCP), with a higher frequency of iatrogenic errors, including a tendency for canal straightening (Abou-Rass, Ellis, 1996; Limongi, et al., 2004).
In general, reducing the amplitude of the movement toward a smaller oscillation with a higher frequency decreased the incidence of iatrogenic errors but was still more of a problem than when using SS files manually to prepare canals (Turek, Langeland, 1982; Harty, Stock, 1974; Hülsmann, Gambal, Bahr, 1999; Bolanos, et al., 1988; Lehman, Gerstein, 1982; O’Conell, Brayton, 1975; Teodorovic, Ivanovic, 1998; Cheung, Chan, 1996; Nagy, et al., 1997; Smith, Edmunds, 1997; Hülsmann, Rummelin, Schäfers, 1997; Petschelt, et al., 1994).
The other common observation after RCP with mechanical SS files was that increasing the size of the preparation risked a higher incidence of procedural errors (Hülsmann, Gambal, Bahr, 1999; Bolanos, et al., 1988; Lehman, Gerstein, 1982; O’Connell, Brayton, 1975; Teodorovic, Ivanovic, 1998; Cheung, Chan, 1996; Nagy, et al., 1997; Smith, Edmunds, 1997; Hülsmann, Rummelin, Schäfers, 1997; Petschelt, et al., 1994; Abou-Rass, Jastrab, 1982; Ianno, Weine, 1989).
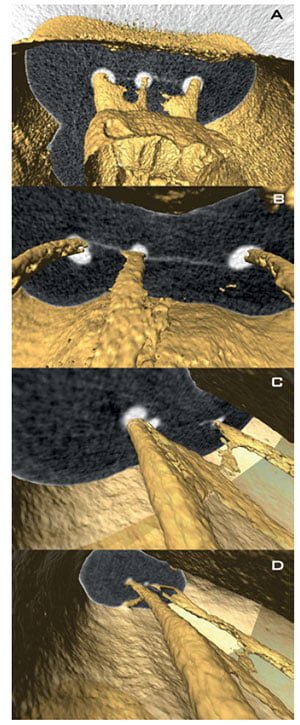
bi-dimensional sections at coronal. B-C. Superimposition of preoperative three-dimensional reconstruction and postoperative
bi-dimensional sections at coronal middle and apical level. D. Showing the modification of root canal anatomy and geometry induced by reciprocating instrumentation
Other studies have also reported procedural errors linked to metal stiffness and restoring force of SS and worse results compared to nickel-titanium instrumentation systems (Hilaly Eid, Wanees, Amin, 2011; Ceyhanli, et al., 2014).
The modern use of SS files in reciprocation
Although there are many systems on the market, the tendency is to limit use to the scouting phase prior to shaping procedures to obtain a glide path. This would minimize the adverse effects of SS files, especially in larger more rigid sizes. Despite the widespread use of mechanical SS files, there is still a lack of scientific evidence on their efficacy (Limpngi, et al., 2004).
SS files used for glide path management should be used with equal 30° forward and backward movement in a reciprocating handpiece (M4 Safety™ Handpiece, SybronEndo/Kerr). The primary observations regarding small SS files for glide path management seem to be promising, but studies are lacking on how they would fare in calcified, curved, and complex canals (Peters, Paque, 2010).
The birth of modern reciprocation for nickel-titanium files of greater taper
Studies have demonstrated the potential in using greater taper nickel-titanium files in shaping the root canal even in the most challenging of anatomical complexities (Hülsmann, Peters, Dummer, 2005; Parashos, Messer, 2006).
However, fracture of nickel-titanium rotary instruments continues to be of concern (Best, et al., 2004) and appears to be a manifestation of continuous rotation. In 2004, one study investigated the endurance limit of nickel-titanium files (Best, et al., 2004); this is the level of stress or strain at which the file can be subjected to before separating (Lindeburg, 1999). This value is a specific deflection angle (DA), characteristic of each instrument; it depends on the size and design features of the instrument.
Every time a rotating file cuts dentin in a constricted canal, torsional deformation develops on its axis. If the deformation is within the plastic limit of the metal, there are no structural changes. However, if repeated cyclic axial deformation accrues, the instrument will fracture due to torsional fatigue, and this is in addition to the flexural fatigue that develops within a curved canal (Pedulla, et al., 2015).
Limiting the angle of rotation in the cutting direction under the endurance limit of the instrument led to the development of a movement that could be defined as partial or asymmetrical reciprocation (Figure 1), in which the angle of rotation in the cutting direction is higher than the angle of rotation in the opposite non-cutting direction. After a certain number of cutting cycles, the instrument would complete a full rotation. When first introduced (Yared, 2008), an ATR Tecnika motor (ATR, Pistoia, Italy) was programmed for this asymmetrical motion, and the file used was a ProTaper® F2 (Dentsply Maillefer). The angles used were described as fourteenth of a circle (144°) in the clockwise (CW) cutting direction and two-tenths of a circle (72°) in the counter-clockwise (CCW) non-cutting direction with a speed of 400 rpm. The technique showed promising results (Malentacca, Lalli, 2002).
The overall speed of this kind of rotational reciprocation is much lower than the speed used for symmetric oscillating reciprocation. Consequently, the rotating effect given by the net difference between CW and CCW movements maintains an adequate cutting efficiency and an apical progression of the instrument while reducing torsional stress.

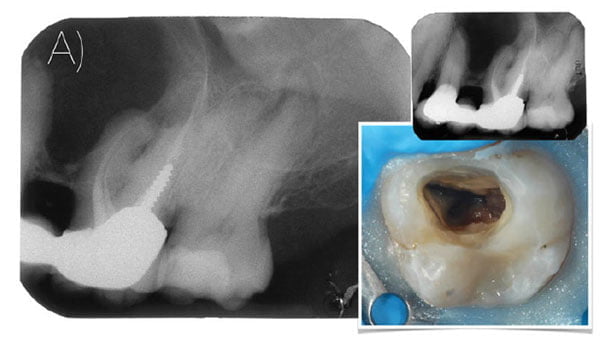
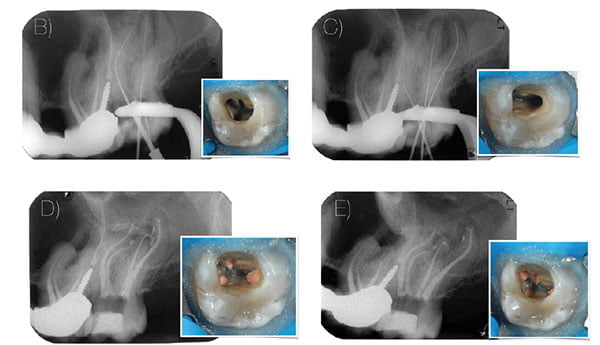
It has been speculated that this kind of reciprocation is similar to the manual balanced force technique as described by Roane and colleagues in 1985. The dynamics enables the instrument to remain centered in the canal, as the cutting force is equal on the concave and convex side of the canal curvature (Figures 2, 3, and 4). Torsional stresses, which are developed on the shank of the file during the cutting action, are reduced as the rotation is under the ideal limit of the DA specific for the file.
This novel asymmetrical movement led to the development of dedicated reciprocating single file (RSF) systems and a new technique where only one file is needed to fully shape a canal to length.
Initial canal negotiation with small (0.08 mm, 0.10 mm tip diameter) SS scouting files allows the clinician to determine the size of the RSF, which will shape the canal (De-Deus, et al., 2010a, 2010b). This approach can be risky for files used in complete rotation because if the file exhibits “taper lock” in the canal, immediate fracture could occur (Yared, 2008). This modified CW/CCW movement led to nickel-titanium files specifically designed for the use in partial reciprocation, such as WaveOne® (Dentsply Maillefer) and Reciproc® (Dentsply VDW).
The files are used with different angles in the cutting and non-cutting direction of 150°/30° (Reciproc with an average
speed of 300 rpm and WaveOne with an average speed of 350 rpm) and that are within their characteristic endurance limit (Webber, 2015).
Actual and set values of the asymmetrical reciprocating movement of different motors were assessed because variables, such as the delay between the two directions of movement and the acceleration to reach the desired speed, could play an important role in the efficacy of the different instruments (Fidler, 2014). Additional studies are needed to explore this variable. For commercial reasons, the flutes of reciprocating files are manufactured in a backward direction so that the CCW movement is greater than the CW movement; and after three cutting cycles, the instrument completes a full reverse rotation. All commercially available nickel-titanium files rotate in a CW direction (Fidler, 2014). Both commercially available RFs are marketed as single file techniques after initial scouting of the canal to determine the correct file size to use to obtain the final shape. A single RSF produces a shape that traditionally would be obtained after a series of three or more rotary nickel-titanium files. The favorable results of reciprocating files indicate their potential as viable alternatives to rotary file systems. Occasionally, it might be necessary to use additional instruments to initially establish the glide path or clean the apical third and the fins of the RCS (Baugh, Wallace, 2005).
An RSF is subjected to a certain amount of mechanical stress during use that otherwise would be distributed among a series of different rotary files. For this reason, manufacturers urge single-use for RSF techniques to prevent the increased risk of file separation in case of multiple usages (Yared, 2008).
Recently, WaveOne has been upgraded to WaveOne Gold. The kinematic of this system is unchanged, but the cross section, size, and geometry of the files have been modified to make the file more flexible and efficient. Gold heat treatment is a proprietary Dentsply post-manufacturing heat treatment process unlike M-Wire, which is a pre-
manufactured heat treatment process. The Gold heat treatment process improves flexibility (Shen, et al., 2013) and allows the instrument to be pre-curved, an advantage when placing the file into canals in more difficult-to-reach posterior regions (Figure 5). Reciproc (Dentsply VDW) is marketed as a file that can prepare the coronal and middle thirds of the root canal without the establishment of an initial glide path (Yared, Ramil, 2013). This procedure has been shown to be clinically successful and safe even in complex canals (De-Deus, et al., 2013) when the clinician follows the manufacturer’s directions for use (Plotino, Grande, Porciani, 2015).
TF™ Adaptive files and the dedicated Elements™ Motor (SybronEndo) have recently been launched. The motor changes its kinematics from a rotating movement (600° CW horizontal rotational motion and 0° CCW) to partial reciprocation (370° in a CW cutting direction and 50° in the non-cutting direction). The change to reciprocation is dependent on the torque to which the file is subjected. The average speed of the RM is not declared by the manufacturer. This type of movement could be defined as a hybrid reciprocation.
Recently, Morita (Japan) has introduced the Root ZX® II OTR Module, a low-speed handpiece where the torque is automatically measured during file rotation. The manufacturer claims that if the torque is less than the set value, the file rotation continues; but if the torque has reached the set value, the file reverses rotation by 90° and then continues in the cutting direction once again. This type of movement could be also defined as a hybrid reciprocation. The clinician has the advantage of continuous rotation when needed, and reciprocating movement in a reverse direction activated by the torque measurement. If too much force is applied, the handpiece will continue reading a torque limit over the set value, and the reciprocating movement will continue.
More recently, several motors have come to market with the functionality to adjust both forward and backward angle of reciprocation, as well as the speed of movement. Theoretically, any instrument on the market could be used in an asymmetrical reciprocation with these motors, but studies are still lacking on how they would perform in terms of safety and quality of the preparation.

Due to the increased popularity of RM and reciprocating files usage, numerous studies have been conducted mainly investigating the mechanical properties, shaping ability, preservation of the root canal anatomy, shaping time, cleaning effectiveness, microcrack formation, bacterial reduction, extrusion of debris, and removal of root canal filling materials. The conclusions from the literature can be summarized as follows (Plotino, et al., 2015):
- Reciprocation extends the lifespan of all types of files tested.
- The amplitude of reciprocation has a significant influence on the cyclic fatigue life of the files tested.
- Reciprocation does not reduce the cutting efficiency of the files tested.
- Reciprocating and rotary motion have similar cutting efficiency.
- Reciprocating files shape canals well and preserve the original canal anatomy.
- The cleaning effectiveness of reciprocating files is comparable to full rotary file sequence systems. Further studies should be conducted to understand the respective influence of the kinematics, the file design, and the number of instruments needed to fully shape canals.
- Reciprocating single file usage reduces the shaping time compared to a full sequence rotary system.
- Dentin microcracks occur independently of the type of file and its kinematics.
- The results of published studies show that the use of reciprocating files would lead to fewer or an equivalent amount of dentin microcracks compared with full sequence rotary systems.
- RFs can promote significant bacterial reduction, but like rotary full sequence systems, they are not able to completely disinfect the RCS.
- The ability of RFs to extrude less debris than rotary files remains a matter of debate.
- Reciprocating files are effective in removing root canal filling material in less time as compared to rotary files, yet no system is able to remove the filling material completely from the RCS.
Conclusion
RM, defined as a repeated backward and forward (clockwise/counter-clockwise) movement, has been extensively used in endodontics for many years and can be applied to many endodontic files.
There are many variations of RM, including:
- Complete reciprocation (oscillation)
- Partial reciprocation (rotational effect)
- Hybrid reciprocation (combined movements)
Hybrid reciprocation can be fixed or flexible — i.e., it can shift from one type of reciprocation to the other in the canal based on mechanical resistance and torque.
It must be borne in mind, however, that no file system is able to completely clean the canal, totally eliminate sessile and planktonic microorganisms, or remove the filling material completely from the root canal system. However, the favorable results of RFs, especially their safety and low rate of fracture, indicate their potential as viable alternatives to rotary file systems (Figures 6 and 7).
References
- Abou-Rass M, Ellis MA. A comparison of three methods of hand and automated instrumentation using the CFS and M4 for preparations of curved and narrow simulated root canals. Braz Endod J. 1996;1:25-33
- Abou-Rass M, Jastrab RJ. The use of rotary instruments as auxiliary aids to root canal preparation of molars. J Endod. 1982;8(2):78-82.
- Baugh D, Wallace J.The role of apical instrumentation in root canal treatment: a review of the literature. J Endod. 2005;31(5):333-340.
- Best S, Watson P, Pilliar R, Kulkarni GG, Yared G. Torsional fatigue and endurance limit of a size 30.06 ProFile rotary instrument. Int Endod J. 2004;37(6):370-373.
- Ceyhanli KT, Erdilek N, Tatar I, Cetintav B. Comparative micro-computed tomography evaluation of apical root canal transportation with the use of ProTaper, RaCe and Safesider systems in human teeth. Aust Endod J. 2014;40(1):12-16.
- Cheung GS, Chan AW. An in vitro comparison of the Excalibur handpiece and hand instrumentation in curved root canals. J Endod. 1996;22(3):131-134.
- De-Deus G, Moreira EJ, Lopes HP, Elias CN. Extended cyclic fatigue life of F2 ProTaper instruments used in reciprocating movement. Int Endod J. 2010a;43(12):1063-1068.
- De-Deus G, Brandão MC, Barino B, Di Giorgi K, Fidel RA, Luna AS. Assessment of apically extruded debris produced by the single-file ProTaper F2 technique under reciprocating movement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010b;10(3):390-394.
- De-Deus G, Arruda TE, Souza EM, Neves A, Magalhães K, Thuanne E, Fidel RA. The ability of the Reciproc R25 instrument to reach the full root canal working length without a glide path. Int Endod J. 2013; 46(10):993-998.
- Dihn Q. An in-vitro evaluation of the Giromatic instrument in the mechanical preparation of root canals. [Thesis]. Minnesota: Univ. of Minnesota;1972.
- Fidler A. Kinematics of 2 reciprocating endodontic motors: the difference between actual and set values. J Endod. 2014;40(7):990-994.
- Frank AL. An evaluation of the Giromatic endodontic handpiece. Oral Surg Oral Med Oral Pathol. 1967;24(3):419-421.
- Grande NM, Ahmed HM, Cohen S, Bukiet F, Plotino G. Current Assessment of Reciprocation in Endodontic Preparation: A Comprehensive Review-Part I: Historic Perspectives and Current Applications. J Endod. 2015;41(11): 1778-1783.
- Harty FJ, Stock CJ. The Giromatic system compared with hand instrumentation in endodontics. Br Dent J. 1974;137(6):239-244.
- Hilaly Eid GE, Wanees Amin SA. Changes in diameter, cross-sectional area, and extent of canal-wall touching on using 3 instrumentation techniques in long-oval canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(5):688-695.
- Hülsmann M, Gambal A, Bahr R. An evaluation of root canal preparation with the automated Excalibur endodontic handpiece. Clin Oral Investig. 1999;3(2):70-78.
- Hülsmann M, Rummelin C, Schäfers F. Root canal cleanliness after preparation with different endodontic handpieces and hand instruments: a comparative SEM investigation. J Endod. 1997;23(5):301-306.
- Hülsmann M, Peters OA, Dummer PM. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Top. 2005;10:30-76.
- Ianno NR, Weine FS. Canal preparation using two mechanical handpieces: distortions, ledging, and potential solutions. Compendium. 1989;10(2):100-102,104-105.
- Kim HC, Kwak SW, Cheung GS, Ko DH, Chung SM, Lee W. Cyclic fatigue and torsional resistance of two new nickel-titanium instruments used in reciprocation motion: Reciproc versus WaveOne. J Endod. 2012;38(4):541-544.
- Jungmann CL, Uchin RA, Bucher JF. Effect of instrumentation on the shape of the root canal. J Endod. 1975;1(2):66-69.
- Lausten LL, Luebke NH, Brantley WA. Bending and metallurgical properties of rotary endodontic instruments. IV. Gates Glidden and Peeso drills. J Endod. 1993;19(9):440-447.
- Laws AJ. Preparation of root canals: an evaluation of mechanical aids. NZ Dent J. 1968;64:156.
- Lehman JW 3rd, Gerstein H. An evaluation of a new mechanized endodontic device: the Endolift. Oral Surg Oral Med Oral Pathol. 1982;53(4):417-424.
- Limongi O, Klymus AO, Baratto Filho F, Vanni JR, Travassos R. In vitro evaluation of the presence of apical deviation with employment of automated handpieces with continuous and alternate motion for root canal preparation. J Appl Oral Sci. 2004;12(3):195-199.
- Lindeburg MR. Civil Engineering Reference Manual for the PE Exam. 7th ed. Belmont, California: Professional Publications Inc.; 1999.
- Luebke NH, Brantley WA. Physical dimensions and torsional properties of rotary endodontic instruments. 1. Gates Glidden drills. J Endod. 1990;16(9):438-441.
- Klayman SM, Brilliant JD. A comparison of the efficacy of serial preparation versus Giromatic preparation. J Endod. 1975;1(10):334-337.
- Malentacca A, Lalli F. Use of nickel titanium instruments with reciprocating movement. Italian Journal of Endodontics. 2002;6:79-84
- Martin H. Ultrasonic disinfection of the root canal. Oral Surg Oral Med Oral Pathol. 1976;42(1):92-99.
- Molven O. A comparison of the dentin-removing ability of five root canal instruments. Scand J Dent Res. 1970;78(6):500-511.
- Nagy CD, Bartha K, Bernath M, Verdes E, Szabo J. A comparative study of seven instruments in shaping the root canal in vitro. Int Endod J. 1997;30(2):124-132.
- O’Connell DT, Brayton SM. Evaluation of root canal preparation with two automated endodontic handpieces. Oral Surg Oral Med Oral Pathol. 1975;39(2): 298-303.
- Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod. 2006; 2(11): 1031-1043.
- Pedullà E, Lo Savio F, Boninelli S, Plotino G, Grande NM, Rapisarda E, La Rosa G. Influence of cyclic torsional preloading on cyclic fatigue resistance of nickel-titanium instruments. Int Endod J. 2015; 48(11):1043-1050.
- Peters OA, Paque F. Current developments in rotary root canal instrument technology and clinical use: a review. Quintessence Int. 2010;41(6):479-488.
- Petschelt A, Krämer N, Reinelt C, Ebert J. Apically extruded material after manual and mechanical root canal instrumentation. J Dent Res. 1994;73:216.
- Powell SE, Simon JH, Maze BB. A comparison of the effect of modified and nonmodified instrument tips on apical canal configuration. J Endod. 1986;12(7): 293-300.
- Plotino G, Grande NM, Porciani PF. Deformation and fracture incidence of Reciproc instruments: a clinical evaluation. Int Endod J. 2015;48(2): 199-205.
- Plotino G, Ahmed HM, Grande NM, Cohen S, Bukiet F. Current Assessment of Reciprocation in Endodontic Preparation: A Comprehensive Review-Part II: Properties and Effectiveness. J Endod. 2015;41(12): 1939-1950.
- Roane JB, Sabala CL, Duncanson MG Jr. The “balanced force” concept for instrumentation of curved canals. J Endod. 1985;11(5):m203-211.
- Sargenti A. Engine powered canal preparation. Addendum to Endodontics. Locarno (Switzerland):AGSA Publication Scientifiques;1974.
- Shen Y, Zhou HM, Zheng YF, Peng B, Haapasalo M. Current challenges and concepts of the thermomechanical treatment of nickel-titanium instruments. J Endod. 2013;39(2): 163-172.
- Smith RB, Edmunds DH. Comparison of two endodontic handpieces during the preparation of simulated root canals. Int Endod J. 1997;30(6): 369-380.
- Teodorovic N, Ivanovic V. Effect of hand, ultrasonic and Excalibur instruments on root canal shaping. Int Endod J. 1998; 31:216-217.
- Turek T, Langeland K. A light microscopic study of the efficacy of the telescopic and the Giromatic preparation of root canals. J Endod. 1982;8(10): 437-443.
- Webber J. Shaping canals with confidence: WaveOne GOLD single-file reciprocating system. Roots. 2015; 1:34-40
- Weine FS, Kelly RF, Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975; 1(8): 255-262.
- Weine FS, Kelly RF, Bray KE. Effect of preparation with endodontic handpieces on original canal shape. J Endod. 1976; 2(10): 298-303.
- Yared G, Ramli GA. Single file reciprocation: a literature review. Endo (Lond Engl). 2013; 7(3): 171-178.
- Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J. 2008;41(4):339-344.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
