Drs. Martin Trope and Gilberto Debelian discuss reaching areas of the canal impossible with standard files
Introduction
 Microbes are the cause of periradicular periodontitis. Root canal treatment is focused on preventing the contamination of the root canal in the treatment of vital (noninfected) tooth or the elimination of microbes when the canal is infected prior to the initiation of treatment. The prevention or elimination of microbes from the root canal poses many challenges.
Microbes are the cause of periradicular periodontitis. Root canal treatment is focused on preventing the contamination of the root canal in the treatment of vital (noninfected) tooth or the elimination of microbes when the canal is infected prior to the initiation of treatment. The prevention or elimination of microbes from the root canal poses many challenges.
[userloggedin]
While the vast majority of the microbes are in the main canal and in the planktonic (loose) form, there are complex anatomical irregularities such as accessory or lateral canals and canal isthmuses intercommunicating with the main canals. In addition, the dentinal walls of the root canal are often covered by biofilm that is particularly difficult to eliminate.
Biofilm in the root canal is structurally the same as dental plaque found on the outside of the root. In periodontics, it is well established that biofilm is infinitely more difficult to remove than the “swimming” planktonic microbes. In fact after many attempts to do otherwise, it is still accepted that periodontal and endodontic biofilm must first be physically disrupted before disinfectants can work on the exposed microbes within the biofilm.
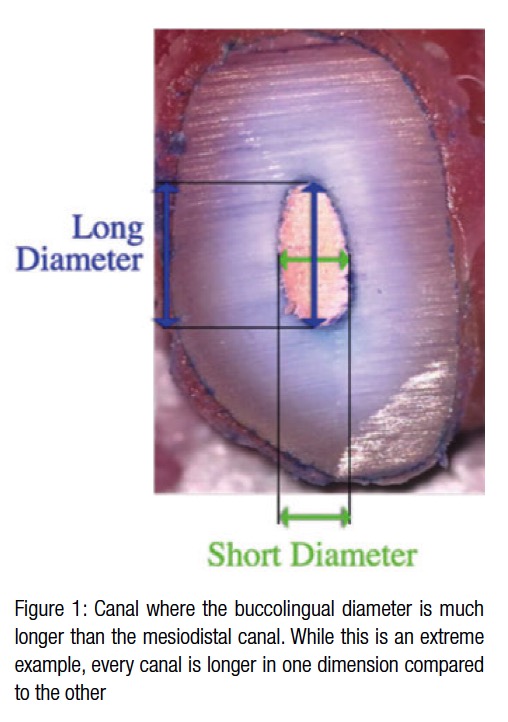
While periodontal scalers are used for physical disruption of plaque in periodontal therapy, root canal therapy relies on the instrumentation of the canal with endodontic files. The major challenge faced in endo-dontics is that almost all canals contain a wider buccolingual dimension compared to the mesiodistal one1 (Figure 1).
 Although there are a multitude of file systems with various metallurgical properties and geometric designs available on the market, they all finally produce a round shape on any given canal cross section (Figure 2). Thus in root canal instrumentation, the practitioner tries to machine a round shape into a non-round canal.
Although there are a multitude of file systems with various metallurgical properties and geometric designs available on the market, they all finally produce a round shape on any given canal cross section (Figure 2). Thus in root canal instrumentation, the practitioner tries to machine a round shape into a non-round canal.
The smaller mesiodistal diameter limits the round files from touching the walls, and thus disrupts biofilm, on the larger buccolingual diameter. Thus it has been considered impossible to safely touch all parts of the canal and disrupt all biofilm in a root canal. If one instruments to the mesiodistal dimension, safety is ensured, and the chances of excessively thinning or perforating the root wall is minimized. However, the bucco-lingual dimension of the canal is likely to still be contaminated (Figure 3).

 In fact, a study by Paqué, et al.,2 found that by using popular instrumentation methods, only 20% to 40% of the canal is touched. If, on the other hand, the longer buccolingual dimension is the aim of instrumentation, the chances of procedural errors in the thin mesiodistal dimension is vastly increased (Figure 3). For these reasons, most practitioners instrument to sizes that they subjectively consider to be safe and add adjunct technologies like passive ultrasonic agitation and negative pressure irrigation to try to disrupt the biofilm without actually physically coming in contact with it.
In fact, a study by Paqué, et al.,2 found that by using popular instrumentation methods, only 20% to 40% of the canal is touched. If, on the other hand, the longer buccolingual dimension is the aim of instrumentation, the chances of procedural errors in the thin mesiodistal dimension is vastly increased (Figure 3). For these reasons, most practitioners instrument to sizes that they subjectively consider to be safe and add adjunct technologies like passive ultrasonic agitation and negative pressure irrigation to try to disrupt the biofilm without actually physically coming in contact with it.
The XP-3D Finisher™ file (Brasseler USA®, Savannah, Georgia) has been recently introduced to the market with a similar aim of the Self-Adjusting File (SAF) — i.e., to contact areas in the longer aspect of the canal for which reach by any round file is not possible. It is used after shaping of the canal with at least a No. 25 size conventional endodontic file.
The XP-3D Finisher instrument is a NiTi file No. 25 without taper, making it extremely flexible and resistant to cyclic fatigue. Below 30°C, it is in its pliable martensite form and can be straightened or manipulated to any shape. Above 35°C (body temperature), it transforms to its austenite phase and is straight until the last 10 mm where it has a spoon shape with a depth of 1.5 mm (Figure 4).
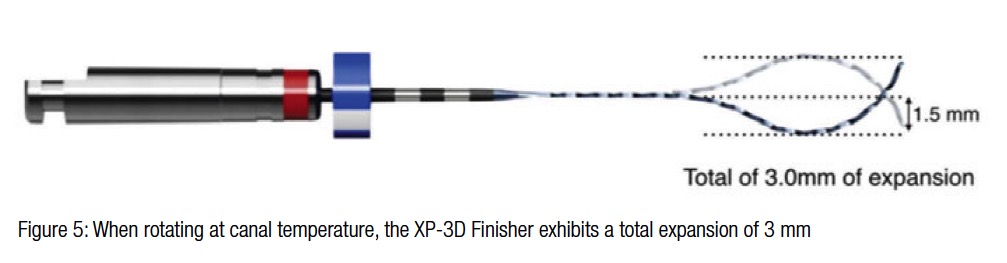
When rotating, this extremely flexible file has a natural diameter of 3 mm in the last 10 mm (Figure 5).
In addition, when the tip is squeezed, the bulb can be expanded to 6 mm; and when the bulb is compressed, the tip will expand to 6 mm.
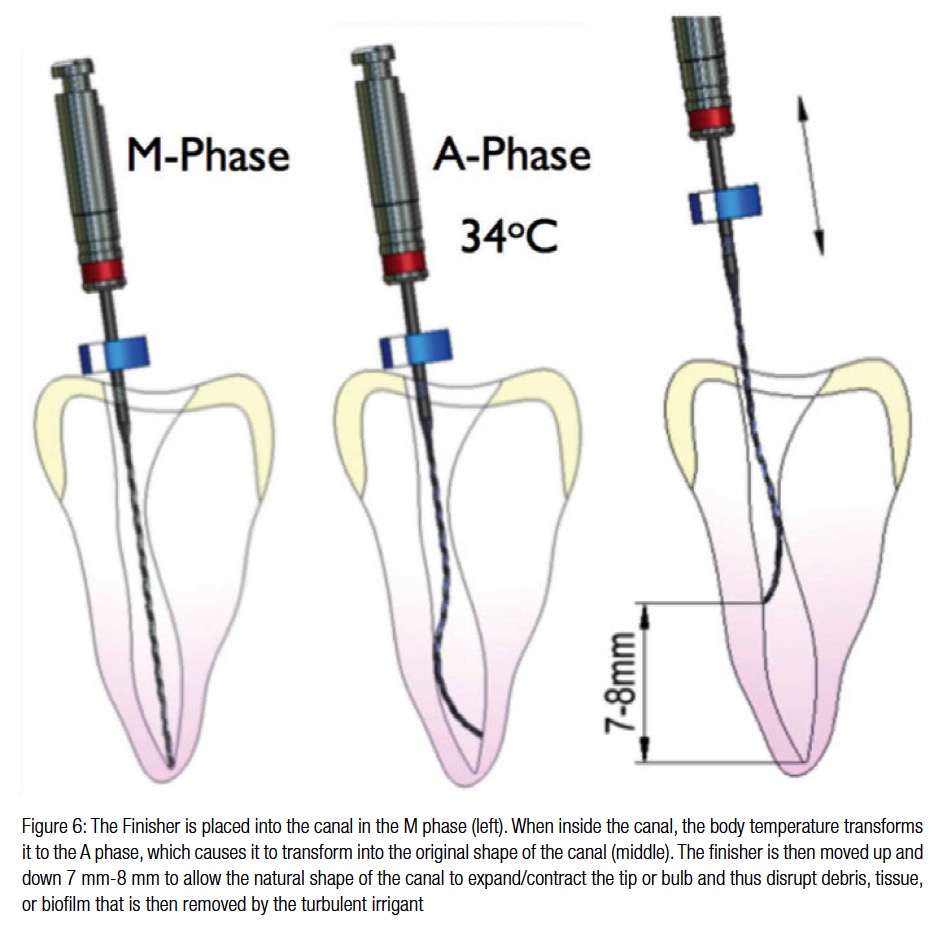
Figure 6 shows the method of use and action of the 3D finisher. It is placed inside the canal while in the most convenient marten-site (pliable) form. When at body temperature or above inside the canal, it will change to the austenite phase and “try” to get to its austenite shape. However, since it is so flexible, it is unable to shape the canal to its shape — instead the canal shapes the file to its shape. When the instrument is now moved up and down for 7 mm to 8 mm inside the canal, the natural constrictions and expansions in the canal will alternately cause the bulb and tip to expand and contract. The action of the tip and the bulb is to scrape and to disrupt the biofilm and, in addition, to cause turbulence of the irrigant for maximal effect on the exposed microbes.
Case examples
 Example 1
Example 1
3D plastic models of mesial canals of mandibular molar cut at 1 mm, 3 mm, 5 mm, and 7 mm from the apex. Group 1 shows the wide buccolingual diameter compared to the mesiodistal diameter at every level. Group 2 shows the roots prepared to size No. 35/.04 with standard round NiTi files. These show that the canals are not cleaned in the buccolingual dimension and also that the round file causes significant thinning of the narrow mesiodistal diameter. Group 3 was instrumented with a small diameter and tapered initial file and finished with the XP-3D Finisher. Here we can see that the original shape of the canal is maintained, and the canal is thoroughly cleaned.
Example 2
In this second example, the distal (left) and mesial (right) canals of an extracted lower molar were viewed with a micro CT preoperatively (left), after initial instrumentation with round files (middle), and after finishing with the XP-3D Finisher (right). As is seen after initial instrumentation with round files, dentinal debris and presumably microbes still remain. These are removed with the 3D finisher without changing the shape of the canal.
Example 3
Tooth with extensive internal root resorption that is impossible to treat with round diameter files without extensive chemical adjunctive therapy. Here the soft tissue is removed in one visit and the canal filled completely, illustrating the effectiveness of the 3D finisher to reach areas that are im-
possible for a standard round file.

 Martin Trope, BDS, DMD, is a Diplomate of the American Board of Endodontics. He has served as Chair of Endodontology, Temple University, Philadelphia, and Chair of Endodontics, University of North Carolina, Chapel Hill. He served as Editor-in-Chief of the journals Dental Traumatology and Endodontic Topics. He is presently in private endodontic practice in Philadelphia and is a Clinical Professor at University of Pennsylvania.
Martin Trope, BDS, DMD, is a Diplomate of the American Board of Endodontics. He has served as Chair of Endodontology, Temple University, Philadelphia, and Chair of Endodontics, University of North Carolina, Chapel Hill. He served as Editor-in-Chief of the journals Dental Traumatology and Endodontic Topics. He is presently in private endodontic practice in Philadelphia and is a Clinical Professor at University of Pennsylvania.
 Gilberto Debelian, DMD, PhD, received his DMD degree from the University of Sao Paulo, Brazil, in 1987. He completed his specialization in Endodontics from the University of Pennsylvania, School of Dental Medicine, in 1991. He concluded his PhD studies at the University of Oslo, Norway, in 1997 in endodontic microbiology. He is an adjunct visiting professor at the postgraduate program in endodontics, University of North Carolina in Chapel Hill and University of Pennsylvania in Philadelphia. Dr. Debelian maintains a private practice limited to endodontics as well as an advanced endodontic microscopy center, EndoInn, in Bekkestua, Norway. He is an author of books and 50 scientific and clinical papers and is currently a member of the scientific advisory panel for the Journal of Endodontics and Endodontic Practice Today, director of the Oslo Endodontic Study Club, and the vice-president of the Norwegian Endodontic Society. Disclosure: Dr. Trope serves as Clinical Director at Brasseler USA®.
Gilberto Debelian, DMD, PhD, received his DMD degree from the University of Sao Paulo, Brazil, in 1987. He completed his specialization in Endodontics from the University of Pennsylvania, School of Dental Medicine, in 1991. He concluded his PhD studies at the University of Oslo, Norway, in 1997 in endodontic microbiology. He is an adjunct visiting professor at the postgraduate program in endodontics, University of North Carolina in Chapel Hill and University of Pennsylvania in Philadelphia. Dr. Debelian maintains a private practice limited to endodontics as well as an advanced endodontic microscopy center, EndoInn, in Bekkestua, Norway. He is an author of books and 50 scientific and clinical papers and is currently a member of the scientific advisory panel for the Journal of Endodontics and Endodontic Practice Today, director of the Oslo Endodontic Study Club, and the vice-president of the Norwegian Endodontic Society. Disclosure: Dr. Trope serves as Clinical Director at Brasseler USA®.
- Wu MK, R’oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89(6):739–743.
- Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod. 2010;36(4):703-707.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
