Drs. Martin Trope, Ken Serota, and Gilberto Debelian discuss ways to effectively instrument the natural shape of the canal and improve cleaning

Figure 1A: Multiple file types with multiple cutting geometries ALL resulting in a final round shape in the canal
The ultimate goal of the instrumentation phase of root canal therapy is to develop a sterile canal system before root filling while retaining as much healthy tooth structure as possible. To date, we have not achieved this goal. We strive for this ideal situation with each technological advance.
The introduction of nickel-titanium (NiTi) files was a major breakthrough that resolved many of the instrumentation challenges presented by stainless steel files. Ease of use is a major advantage to the practitioner, and curvatures that were previously considered impossible, or limited to highly skilled specialists, are now considered fairly routine. However, many challenges remain to achieve the ultimate goal of root canal instrumentation regardless of whether stainless steel or NiTi instruments are used.
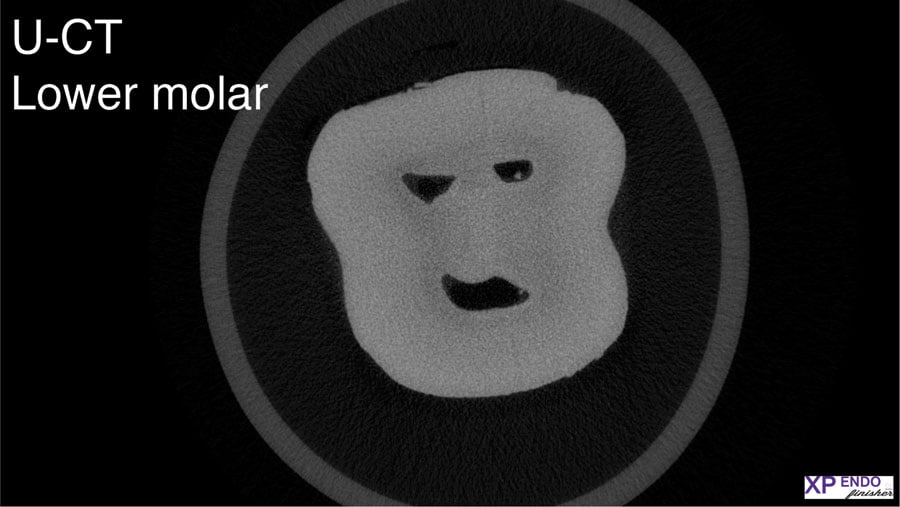
Figure 1B: CBCT cross section of a mandibular molar in the mid-root area. None of the canals are round
Challenges of traditional files
1.The major problem of today’s files is that whatever the cutting geometry, they all produce a round shape ignoring the obvious; a root canal is not round (Figures 1A and 1B).1
Therefore, it is impossible to shape the interfacial dentin of the canal unless the file chosen corresponds to the largest diameter of the non-round canal. As the root shape mimics the canal shape, this is impossible to achieve. The small diameter of the root will invariably be severely compromised or even perforated with this approach (Figure 2).
Historically, this limitation has been hidden from view (and consciousness) since a typical periapical radiograph shows the narrower M-D dimension of the canal.2 For this reason, cleaning to the narrower diameter appears adequate on the posttreatment radiograph. However, 3D axial radiographs using CBCT have brought this fact into clear view (Figure 1B). Mapping of the root canal space magnified by micro-CT analyses show that the typical round file used in this way touches less than 50% of the canal wall3 (Figure 3).

Figure 2: Because the root shape mimics the canal shape, making a round shape using the maximum diameter is clinically not practical
2.Perhaps, one of the most under-appreciated challenges of round files is that while in use, they create a large amount of dentinal debris. Traditionally, our focus has been on the debris pushed through the apex during instrumentation, assuming that the rest of the debris moves coronally and is flushed from the canal. It has never been appreciated that this debris is first pushed into all the non–round parts of the canal blocking these areas to further cleaning and disinfection by adjunctive cleaning methods and irrigation solutions4,5 (Figure 4).
Additionally, when all these irregularities are compacted with debris, any further debris created will cause increased pressure on the root with the possible development of micro fractures. The current trend of fewer files and larger tapers exacerbates this potential fracture problem.
In summary, endodontic files have been used to make an artificial round shape in a non-round canal. Additionally, we fill the non-round parts of the canal with debris, further hampering our ability to control the microbes within the canal. The increasing pressure on the walls of the canal potentially predisposes the root to future root fracture.

Figure 3: Walls touched when a round file to the minimum diameter is used. Less than 50% of the canal walls are touched.
Solving the challenges utilizing the properties of NiTi metals
Ideally, instead of creating an artificial shape in the canal, technology should be used to design a file that adapts to the natural anatomy of the root canal space.
The breakthrough instrument that showed this potential was the Self-Adjusting File (SAF, ReDent Nova, Ltd., Ramat Gan, Israel). This file is made of NiTi metal according to the principles used in a medical stent. If squeezed in one direction, it expands in the other direction. As the canal is narrow in the M-D dimension and wider in the B-L dimension, this principle works in the root canal space as well.6
 Figure 4: Irregular canal after instrumentation with a round file. Note the debris pushed into the irregularities of the canal(Courtesy of Dr. G. De Deus)
Figure 4: Irregular canal after instrumentation with a round file. Note the debris pushed into the irregularities of the canal(Courtesy of Dr. G. De Deus)
Recently, instruments developed to remove canal contents three dimensionally have been included into the endodontic armamentarium. In addition, these revolutionary instruments remove as little healthy tissue as possible. (XP-3D Shaper™/Finisher, Brasseler USA®, Savannah, Georgia).
The XP-3D Shaper was designed to create a basic shape in the canal while respecting the original anatomy of the root canal space without packing debris into untouched areas. The XP-3D finisher has a “reach” of at least 3 mm, thereby touching even the widest canal diameters while not changing the original shape of the canal.
XP-3D Shaper
The Shaper file has a diameter of 0.30 mm at the tip and 0.01 taper (#30/01). The small taper makes the file highly flexible and resistant to cyclic fatigue (Figure 5A).
The file has a Booster tip (BT) that allows it to move from a glide path of 15/02 or 10/04 immediately to a minimum diameter of 0.30 mm. At room temperature, the file has a slight serpentine shape, and it is the Martensite form that allows it to be bent and manipulated to any desired shape. However, at body temperature in the canal, it changes to the Austenite form and has the expansion capacity to create a 0.08 taper when no resistance is met (in air) or when working to overcome the resistance of the dentin (Figures 5A and 5B).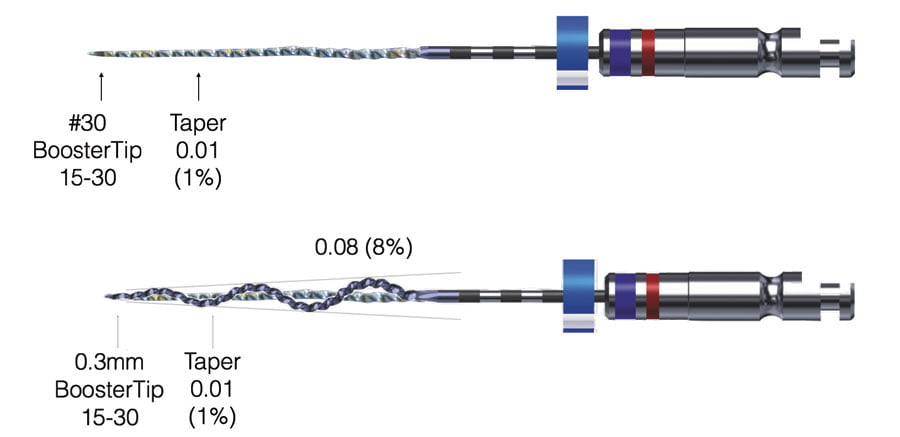
Figures 5A and 5B: (top) The basic dimensions of the file. (bottom) The file at body temperature in the full Austenite form with no resistance. The file has a serpentine shape with a 0.08 taper
Figure 6: The file at room temperature in the Martensite phase. The file is malleable and bendable, so it can be pre-bent to assist in placing in the canal
In tight canals, the XP-Shaper will be squeezed down close to its minimum diameter of 30/01 and then dependent on the time that it works inside the canal, it will expand its taper to the needs or requirements of each individual practitioner.
To better explain the unique properties of the file, the following should be understood:
1.At room temperature, the Shaper is in the Martensite phase, enabling it to be bent and more readily placed in the canal (Figure 6).
2.The Booster (BT) tip is analogous to a very finely sharpened lead pencil (Figure 7).
The “lead” non-cutting section enters the canal into the pre-established narrow (15/02 or 10/04) glide path, ensuring precise guidance and centering of the instrument. There are no cutting flutes on this section, and the instrument slips into the prepared apical component of the glide path to a depth of ¼ mm. The next ¼ mm section of the Booster tip is configured with six cutting flutes at a pre-set angle. Rotation of these flutes sizes the next ¼ of a mm of the canal space from a 0.15 mm to a 0.3 mm diameter. Going from the glide path sizes to size No. 30 should require no more than 3 to 5 easy long up/down strokes.
The 0.3 mm diameter has been chosen in order to enable a No. 31 gauge irrigating needle to reach the working length, thereby maximizing irrigation efficiency and the creation of a shelf for seating the GP point when filling the root canal.
3.The file has the capacity to expand from taper of 0.01 to 0.02/0.04/ 0.06/0.08 while still maintaining the flexibility of the original 0.01 taper (Figure 8).

Figure 7: SEM picture of the booster tip. (top) The first 0.25 mm comes to a sharp point and is non-cutting. The next 0.25 mm has six cutting flutes at a pre-set angle. (bottom) View looking down at the BT tip. The tip is extremely small and is used as a glide file. The six cutting flutes start at 0.15 mm and end at 0.3 mm
Figure 8: Illustration showing the decreased flexibility of files with the same tip size but increasing tapers. The XP Shaper maintains the flexibility of the 0.01 taper but has the cutting capacity of 0.04 or above
At body temperatures, the file attains its Austenite characteristics and attempts to achieve its 0.08 taper. However, it has to overcome any resistance that may be present in the canal in order to do this. Therefore, in a very tight canal, approximately every 10 long strokes will achieve a 2% increase in taper. As we want to maintain as much healthy tissue as possible, it is recommended that when the working length has been achieved in the first 3 to 5 strokes, an additional 10 long strokes will achieve a 0.04 taper, which is sufficient to adequately disinfect the canal. In naturally larger canals, the file easily reaches larger tapers without having to overcome dentin resistance. As a function of its serpentine shape, light brushing and up to 30 long strokes will result in over 90% of the walls being touched in these larger non-complex canals (Figure 9).
4.The file is adaptive to the original shape of the canal. As described in Figure 5, the file has a serpentine shape. The space available for this shape in motion enables a light brushing to touch 90% or more of the walls in larger non-complex canals (Figure 9).
5.Round files packing debris into the canal irregularities is a major problem in sufficiently cleaning a canal. One of the major advantages of the Shaper is that the serpentine shape and 0.01 taper of the file allows space in the canal for the debris to be maintained in solution and effectively irrigated and removed from the canal (Figure 10).
The debris is NOT pushed into irregularities; rather, it is effectively removed from the canal. This enables additional adjuncts to work maximally after the initial shape is achieved. Tests show that pressure is not built up using the Shaper (Figures 11A and 11B). The concern about micro-cracks disappears with the use of this file.7
In summary, the XP Shaper first creates enough space in a canal to effectively and quickly irrigate dentinal and microbial debris from the root canal space. Second, while touching more walls than any round file design, it will maintain the original shape of the canal, not pack debris into the irregularities of the canal, and thus maximize the effectiveness of cleaning adjuncts.8
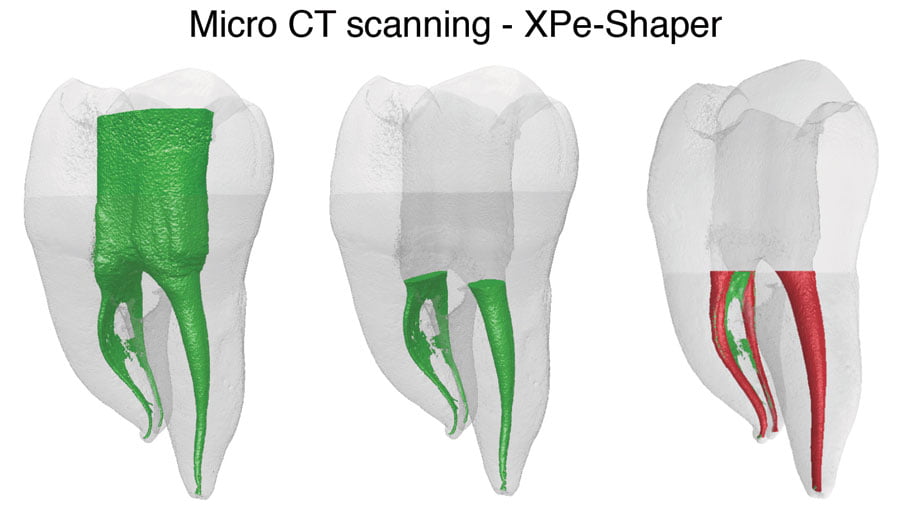
Figure 9: In small canals (mesial canals), the file will first reach a diameter of 0.3 mm and then in time increase the taper of the canal
while maintaining the original anatomy and not packing debris. (See No. 5 on next page.) However, in the distal canal, little resistance
is encountered by the file. Now the serpentine shape and flexibility of the file result in more than 90% of the canal wall being touched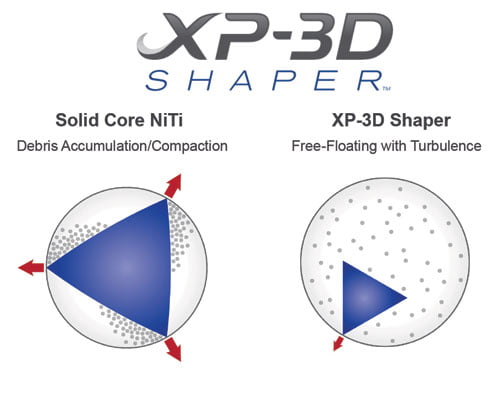
Figure 10: (left) An illustration of cutting with a traditional round file. There is little space for the debris so it will pack into canal irregularities. (right) An illustration showing the Shaper. Here most of the canal is empty so that the debris can stay in solution and NOT be packed. Subsequent irrigation will remove the debris from the canal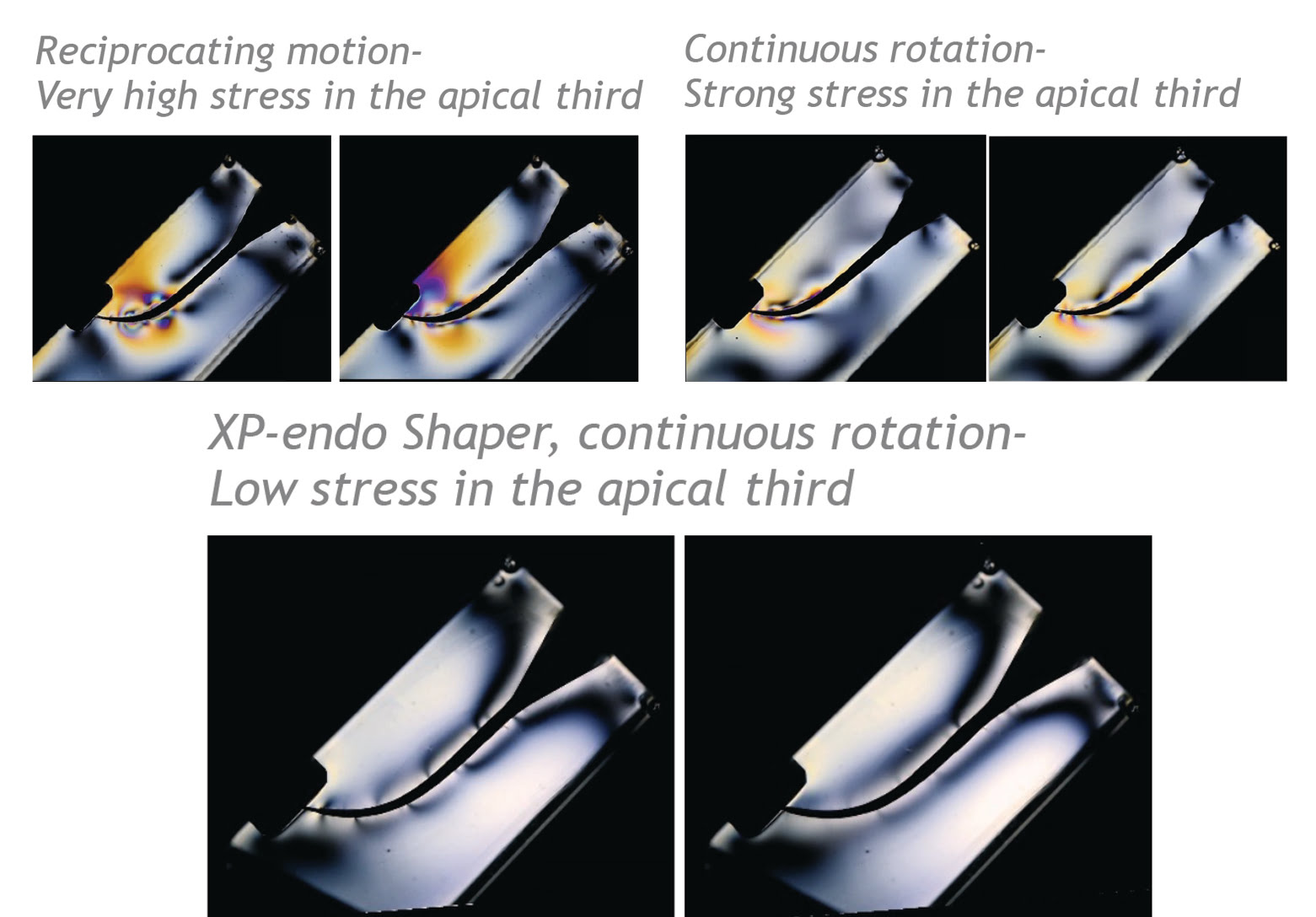
Figure 11A: Plastic blocks with light filters in order to show pressure buildup during instrumentation with different file types. The colors show that reciprocating motion files create the most pressure followed by one-file systems with continuous rotation. The lower picture shows instrumentation with the Shaper file showing no pressure buildup
Retreatment effectiveness
The serpentine shape of the file (hollow or virtual core) and its resistance to cyclic fatigue make it ideal for the removal of the core gutta percha for retreatment procedures. It is recommended that a “starting point” is achieved with a narrow ultrasonic tip or round file and then with the aid of a solvent. The file is used at higher speeds than recommended for primary endodontic treatment. The core GP will often be completely removed, thus decreasing the amount that is pushed into the interfacial dentin and irregularities of the canal space (Figure 12).
XP-3D Finisher
The XP-3D Finisher is a unique instrument with a larger “reach” than the Shaper. This enables it to touch and scrape areas that exceed the reach of the Shaper. Additionally, it will not cut dentin but rather scrape the walls, thus not changing the original shape of the canal.
The dimension of the Finisher is 0.25 mm in diameter (No. 25) with a 0.00 taper.
Again, like the Shaper, in the Martensite form at room temperature, its shape can be manipulated to suit the practitioner. When at body temperature, it immediately achieves a sickle shape in the last 10 mm of the instrument with a depth of 1.5 mm. Thus, when the file is spinning, it has a diameter of 3 mm. However, if the bulb is squeezed, the tip can expand up to 6 mm. Also, if the tip is squeezed, the bulb has the capacity to expand much more than the 3 mm (Figure 13).
When placed into a typical canal and moved up and down, the natural expansion and contraction created by the anatomy of the canal wall will ensure that the tip and bulb can expand and contract into all the irregularities of the canal while not being strong enough to change the original shape before the Finisher is used (Figures 14A and 14B).
In addition, the Finisher creates a robust turbulence of the irrigating solution further enhancing disinfection.
Research indicates that the Finisher is particularly beneficial in the apical third of the canal and is extremely effective in removing dentinal debris. Most importantly, studies show it to be the most effective adjunct in removal of microbes in the main canal and up to 40 microns into the tubules.9-11
Retreatment effectiveness
A retreatment Finisher is available with a core of 0.30 in diameter making it more robust in removing residual gutta percha and debris from the irregularities of the root canal space.
A study by Alves, et al., showed a 69% reduction of debris after initial retreatment with standard round files12 (Figure 16).
In summary, the XP-3D Shaper and Finisher are instruments that can effectively instrument the natural shape of the canal and decrease residual microflora prior to filling the root canal. Equally as important, this improved cleaning is performed without sacrificing healthy root structure, thus maintaining the strength and integrity of the tooth and ultimately its functionality.
The next paper will address slight modification of the shape of the canal to synchronize the fitting of a gutta-percha point and post if required.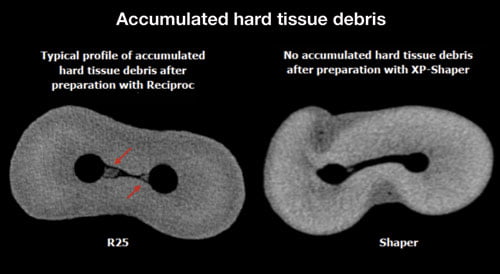
Figure 11B: Micro-CT picture showing debris packing for reciprocating files on left while on the right the Shaper results in no debris packing at all. This could explain the superior effectiveness of the adjunct instru-ments after the use of the Shaper and the increased pressure build up for reciprocating files vs the Shaper file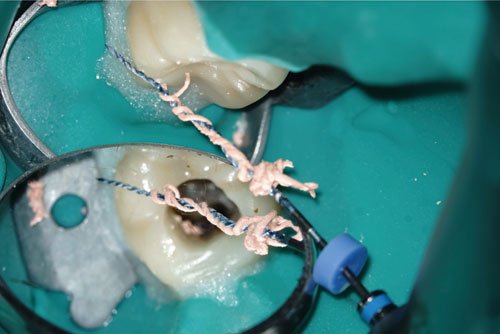
Figure 12: Illustration of the entire gutta-percha core material removed with the use of the 3D-XP Shaper. The serpentine shape of the instrument facilitates the removal of the entire core at once. (Courtesy Dr. K Laudebach)
Figure 13: (Top) The dimensions of the XP-3D Finisher are 0.25 diameter and 0.00 taper. (Bottom) When at body temperature in the Austenite phase, the last 10 mm of the instrument achieves a sickle shape with a depth of 1.5 mm
Figures 14A and 14B: When placed in the canal and moved up and down, the anatomy of the canal will cause the file to expand and contract, thus entering small indentations that cannot be reached by any other files
Figure 15: Picture of a transparent tooth with the XP-3D Finisher cleaning an indentation within the canal due to its sickle shape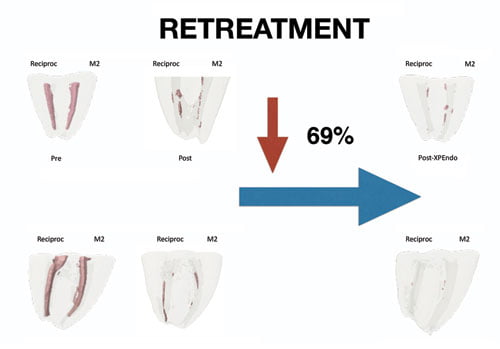
Figure 16: Sixty-nine percent reduction of debris found with the use of the XP-3D Finisher R after standard retreatment with round files
 Martin Trope, BDS, was born in Johannesburg, South Africa, where he received his dental degree in 1976. He practiced general dentistry and endodontics from 1976 to 1980 and then moved to Philadelphia, Pennsylvania, to specialize in endodontics at the University of Pennsylvania. He became chair of endodontology at the School of Dentistry, Temple University in 1989. Dr. Trope is now a clinical professor at the Department of Endodontics, School of Dental Medicine, University of Pennsylvania. He is also in private practice in Philadelphia.
Martin Trope, BDS, was born in Johannesburg, South Africa, where he received his dental degree in 1976. He practiced general dentistry and endodontics from 1976 to 1980 and then moved to Philadelphia, Pennsylvania, to specialize in endodontics at the University of Pennsylvania. He became chair of endodontology at the School of Dentistry, Temple University in 1989. Dr. Trope is now a clinical professor at the Department of Endodontics, School of Dental Medicine, University of Pennsylvania. He is also in private practice in Philadelphia.
 Ken Serota, DDS, MMSc, graduated from the University of Toronto Faculty of Dentistry in 1973 and was awarded the George W. Switzer Memorial Key for excellence in Prosthodontics. He received his Certificate in Endodontics and Master of Medical Sciences Degree from the Harvard-Forsyth Dental Center in Boston, Massachusetts. In 1981, he was the recipient of the American Association of Endodontists Memorial Research Award for his work in nuclear medicine screening procedures related to dental pathology. He provided an interactive endodontic program for the Ontario Dental Association from 1983 to 1997 and was awarded the O.D.A. Award of Merit in 1987 for his efforts in the provision of continuing education. Active in online education since 1998, he is the founder of the online endo forum ROOTS, and the Facebook forums NEXUS. The author of numerous publications, he is on staff at the University of Toronto postdoctoral endodontics department. In private practice from 1981, he is currently on the faculty of the endodontic training Next Level Endodontics in Philadelphia.
Ken Serota, DDS, MMSc, graduated from the University of Toronto Faculty of Dentistry in 1973 and was awarded the George W. Switzer Memorial Key for excellence in Prosthodontics. He received his Certificate in Endodontics and Master of Medical Sciences Degree from the Harvard-Forsyth Dental Center in Boston, Massachusetts. In 1981, he was the recipient of the American Association of Endodontists Memorial Research Award for his work in nuclear medicine screening procedures related to dental pathology. He provided an interactive endodontic program for the Ontario Dental Association from 1983 to 1997 and was awarded the O.D.A. Award of Merit in 1987 for his efforts in the provision of continuing education. Active in online education since 1998, he is the founder of the online endo forum ROOTS, and the Facebook forums NEXUS. The author of numerous publications, he is on staff at the University of Toronto postdoctoral endodontics department. In private practice from 1981, he is currently on the faculty of the endodontic training Next Level Endodontics in Philadelphia.
 Gilberto Debelian, DMD, received his dental degree from the University of Săo Paulo, Brazil, in 1987. He completed his specialization in endodontics at the University of Pennsylvania in 1991. He completed his PhD studies at the University of Oslo in 1997. He is an adjunct visiting professor in the postgraduate programs in endodontics at the University of North Carolina at Chapel Hill and the University of Pennsylvania. Dr. Debelian maintains a private specialist endodontics practice in Bekkestua, Norway.
Gilberto Debelian, DMD, received his dental degree from the University of Săo Paulo, Brazil, in 1987. He completed his specialization in endodontics at the University of Pennsylvania in 1991. He completed his PhD studies at the University of Oslo in 1997. He is an adjunct visiting professor in the postgraduate programs in endodontics at the University of North Carolina at Chapel Hill and the University of Pennsylvania. Dr. Debelian maintains a private specialist endodontics practice in Bekkestua, Norway.
Disclosure: Dr. Trope is a paid consultant for Brasseler. Drs. Serota and Debelian do not have a financial interest in sales from Brasseler.
- Wolf TG, Paqué F, Zeller M, Willershausen B, Briseño-Marroquín B. Root canal morphology and configuration of 118 mandibular first molars by means of micro-computed tomography: an ex vivo study. J Endod. 2016; 42(4):610-614.
- Peters OA, Laib A, Rüegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry using high-resolution computed tomography. J Dent Res. 2000;79(6):1405-1409.
- Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod. 2010;36(4):703-707.
- Paqué F, Al-Jadaa A, Kfir A. Hard-tissue debris accumulation created by conventional rotary versus self-adjusting file instrumentation in mesial root canal systems of mandibular molars. Int Endod J. 2012;45(5):413-418.
- De-Deus G, Belladonna FG, Silva EJ, et al. Micro-CT evaluation of non-instrumented canal areas with different enlargements performed by NiTi systems. Braz Dent J. 2015; 26(6):624-629.
- Metzger Z. From files to SAF: 3D endodontic treatment is possible at last. Alpha Omegan. 2011;104(1-2):36-44.
- Bayram HM, Bayram E, Ocak M, Uygun AD, Celik HH. Effect of ProTaper Gold, Self-Adjusting File, and XP-endo Shaper instruments on dentinal microcrack formation: a micro-computed tomographic study. J Endod. 2017;43(7):1166-1169.
- Azim AA, Piasecki L, da Silva Neto UX, Cruz ATG, Azim KA. XP Shaper, a novel adaptive core rotary instrument: micro-computed tomographic analysis of its shaping abilities [published online ahead of print July 20, 2017]. J Endod. doi: 10.1016/j.joen.2017.04.022.
- Alves FR, Andrade-Junior CV, Marceliano-Alves MF, et al. Adjunctive steps for disinfection of the mandibular molar root canal system: a correlative bacteriologic, micro-computed tomography, and cryopulverization approach. J Endod. 2016;42(11):1667-1672,
- Azim AA, Aksel H, Zhuang T, et al. Efficacy of 4 irrigation protocols in killing bacteria colonized in dentinal tubules examined by a novel confocal laser scanning microscope analysis. J Endod. 2016;42(6):928-934.
- Bao P, Shen Y, Lin J, Haapasalo M. In vitro efficacy of X-endo Finisher with 2 different protocols on biofilm removal from apical root canals. J Endod. 2017; 43(2):321-325.
- Alves F, Marcelano-Alves MF, Sousa JC, et al. Removal of root canal filling in curved canals using either reciprocation single- or rotary multi-instrument system and a supplementary step with the XP-endo Finisher. J Endod. 2016; 42(7):1114-1119.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
