Dr. Allen Ali Nasseh discusses nonsurgical retreatment with innovative instruments
 Nickel titanium has been a miracle alloy in the past few decades. Since its discovery by the Naval Ordinance in 1958 during attempts to develop the ideal alloy for ballistic missile nose cones, to its adaptation in medicine in the 1980s for cardiac stents, and later for endodontic files and orthodontic wires, this alloy has seen lots of modifications.
Nickel titanium has been a miracle alloy in the past few decades. Since its discovery by the Naval Ordinance in 1958 during attempts to develop the ideal alloy for ballistic missile nose cones, to its adaptation in medicine in the 1980s for cardiac stents, and later for endodontic files and orthodontic wires, this alloy has seen lots of modifications.
[userloggedin]
Each modification has aimed to extract the best physical properties for a specific application. The latest patented formulation of this alloy has yielded a unique wire that combined with a unique instrument design, can help solve a very specific, but important endodontic problem — the problem of cleaning oval canals with round endodontic files!
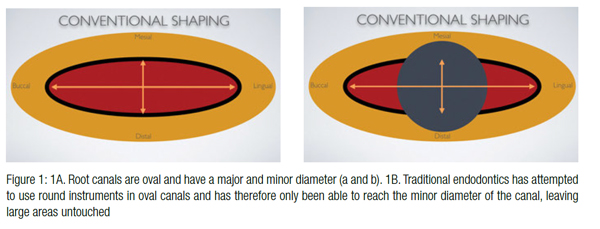
We know that human root canals are primarily oval, possessing a major diameter as a well as a minor diameter. Historically, however, endodontic instruments have evolved to cut round holes in these oval canals (Figure 1). As a result, large areas of the canal have remained untouched despite vigorous instrumentation and irrigation. Furthermore, rotary and reciprocating motions have packed the cut debris from the root canal in the oval areas preventing adequate cleaning and disinfection of
this space.
The application of the newly patented NiTi alloy called MaxWire (Brasseler USA®, Savannah, Georgia) with the special ability to shift crystalline structure at body temperature in order to adapt to the root canal wall, has provided a unique instrument with the promise of anatomical shaping. Anatomical shaping is the process of shaping by enlarging the natural cross-sectional shape of the root in all directions, rather than forcing a round-shaped rotary file into an oval canal, which results in too much cleaning in some areas of the canal and not enough elsewhere.
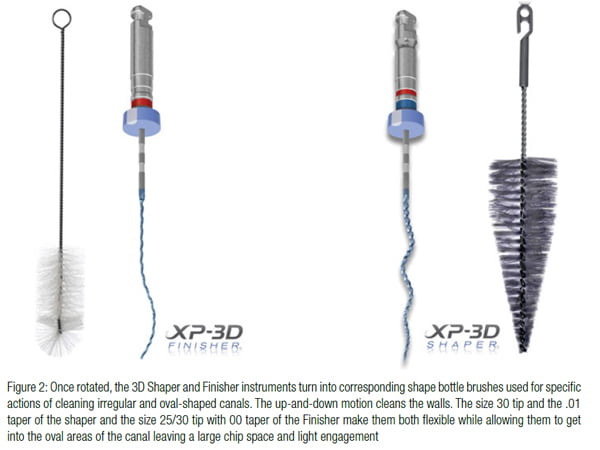 The newly released XP 3-D Shaper and Finisher™ instruments (Brasseler USA, Savannah, Georgia) are unique in their ability to shape canals or enhance irrigation while using the MaxWire’s adaptive core technology. MaxWire alloy has been designed to go through a martensitic transformation at temperatures above 35 degrees Celsius. This temperature represents the body temperature inside the root canal and allows the instrument to shape shift from a relatively straight and very malleable shape at room temperature, where the alloy is in its martensitic phase (M-Phase), to a more robust and serpentine shape at body temperature, when the metal transforms into its austenitic phase (A-Phase). As a result of this temperature-driven transformation, the instrument is more flexible and straight at room temperature but becomes an efficient cutting instrument at body temperature when the file design expands to engage a much wider envelope of motion than the file at room temperature. Both instruments operate at 800-1,000 rpm and can be used on a standard rotary handpiece. The rotation of this adaptive shape at body temperature inside a root canal transforms this instrument into a virtual bottle brush with the capacity of touching the surfaces of the root canal in all directions (Figure 2). Due to its thin core and extreme flexibility (1% taper for the Shaper and no taper for the Finisher instrument), the instrument can fit inside the oval and bounce off the walls touching all surfaces and cutting or scraping dentin. The main difference between the two 3D instruments is that the Finisher essentially functions like a small plastic bottle brush, and the Shaper functions like a tapered metal brush. Therefore, the Finisher scrubs irregularly shaped walls of the root canal during up-and-down motion while the Shaper actually cuts dentin and creates a tapered shape while using the same motion.
The newly released XP 3-D Shaper and Finisher™ instruments (Brasseler USA, Savannah, Georgia) are unique in their ability to shape canals or enhance irrigation while using the MaxWire’s adaptive core technology. MaxWire alloy has been designed to go through a martensitic transformation at temperatures above 35 degrees Celsius. This temperature represents the body temperature inside the root canal and allows the instrument to shape shift from a relatively straight and very malleable shape at room temperature, where the alloy is in its martensitic phase (M-Phase), to a more robust and serpentine shape at body temperature, when the metal transforms into its austenitic phase (A-Phase). As a result of this temperature-driven transformation, the instrument is more flexible and straight at room temperature but becomes an efficient cutting instrument at body temperature when the file design expands to engage a much wider envelope of motion than the file at room temperature. Both instruments operate at 800-1,000 rpm and can be used on a standard rotary handpiece. The rotation of this adaptive shape at body temperature inside a root canal transforms this instrument into a virtual bottle brush with the capacity of touching the surfaces of the root canal in all directions (Figure 2). Due to its thin core and extreme flexibility (1% taper for the Shaper and no taper for the Finisher instrument), the instrument can fit inside the oval and bounce off the walls touching all surfaces and cutting or scraping dentin. The main difference between the two 3D instruments is that the Finisher essentially functions like a small plastic bottle brush, and the Shaper functions like a tapered metal brush. Therefore, the Finisher scrubs irregularly shaped walls of the root canal during up-and-down motion while the Shaper actually cuts dentin and creates a tapered shape while using the same motion.
In this article, I would like to share a recently treated nonsurgical retreatment case where both the 3D Finisher and Shaper were utilized to facilitate and expedite various phases of instrumentation.
A symptomatic mandibular left second molar was referred to for evaluation (Figure 3). Following thorough clinical examination and testing, the tooth was diagnosed with a pulpal diagnosis of previous endodontic therapy with Symptomatic Apical Periodontitis. The probing was normal around the tooth. Although the previous root canal therapy was performed 2 years previously and looked adequate, apicoectomy was deemed risky due to the length of the root and the difficult access to the area. As a result, a nonsurgical retreatment was recommended. The patient accepted the treatment plan, and following mandibular-block anesthesia, the tooth was isolated and access made through the gold crown. The root canal fillings were identified in all canals through the crown, and the coronal half of the gutta percha was removed in each root using an ESX® Orifice Opener (Brasseler USA, Savannah, Georgia) and heat. Chloroform was then used in combination with a descending order of sizes 40-30 ESX® Files (Brasseler USA, Savannah, Georgia) in single stroke and clean motion. Once working length was achieved and measured using EndoSync™ A.I. (Brasseler USA, Savannah, Georgia), patency was confirmed in all three canals, and gutta percha was removed to a size 40/04 ESX File in all canals. Following thorough irrigation and ultrasonic use, some small gutta-percha tags were visible on the canal walls. The canal was then flooded with sodium hypochlorite, and the 3D Finisher R file was used at 800 rpm (1.0Ncm torque) for three 20-second intervals with 4 mm-7 mm-long strokes up and down each canal. Each 20-second interval was followed by irrigation in the canal, where a large amount of debris and shredded gutta percha was observed to irrigate out of the canal. Following this protocol, the gutta-percha tags on the wall that were observed with the microscope but could not be removed with the ultrasonic and conventional instrumentation were no longer visually present.
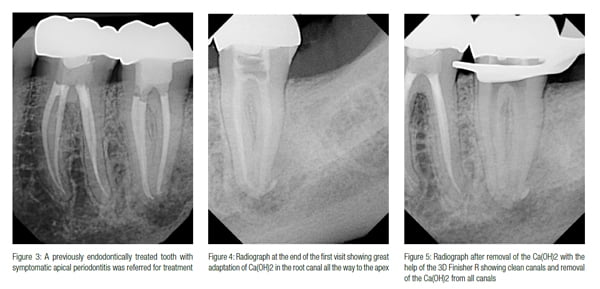 Calcium hydroxide therapy was performed for additional disinfection prior to obturation. The Finisher was also used to take the Ca(OH)2 to the full working length and coat the walls. The instrument was used at a lower rpm (300) to coat the walls, and a postoperative Ca(OH)2 radiograph was taken (Figure 4).
Calcium hydroxide therapy was performed for additional disinfection prior to obturation. The Finisher was also used to take the Ca(OH)2 to the full working length and coat the walls. The instrument was used at a lower rpm (300) to coat the walls, and a postoperative Ca(OH)2 radiograph was taken (Figure 4).
The patient returned 2 weeks later to complete the retreatment procedure. The patient’s symptoms had completely resolved. The patient claimed experiencing no postoperative pain after his first visit. The tooth was isolated and accessed. The calcium hydroxide was removed with irrigation followed by the use of the 3D Shaper to length using the instrument for 20 seconds in each canal followed by irrigation. A radiograph was taken to confirm the removal of the Ca(OH)2 (Figure 5).
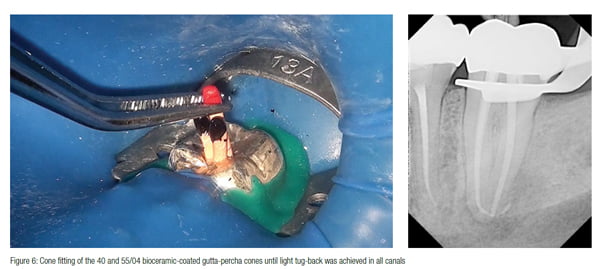
The XP 3D Shaper was then used in each canal for 10 up-and-down strokes. Irrigation confirms removal of additional debris from the root canal. Canals were then dried using paper points, and constant tapered 40 and 55/04 EndoSequence® BC gutta-percha cones (Brasseler USA, Savannah, Georgia) were fitted to length and confirmed radiographically (Figure 6).
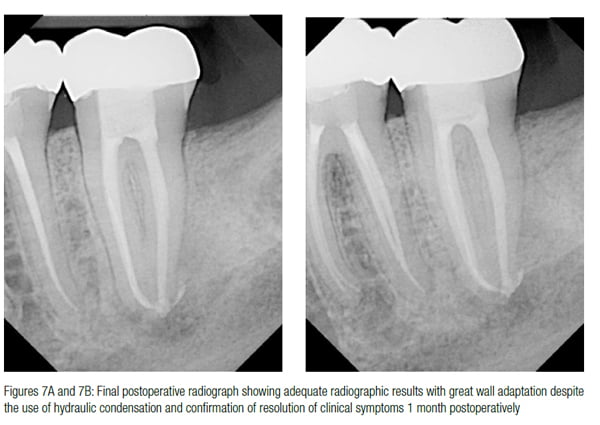
 The cones were then cemented using EndoSequence® BC Sealer™ (Brasseler USA, Savannah, Georgia) to full length and hydraulically condensed after searing off at the orifice. The access was temporized. An immediate and 1 month follow-up radiograph was obtained, and patient’s resolution of clinical symptoms were confirmed (Figure 7). The patient will be monitored for bony healing at 6 months postoperatively.
The cones were then cemented using EndoSequence® BC Sealer™ (Brasseler USA, Savannah, Georgia) to full length and hydraulically condensed after searing off at the orifice. The access was temporized. An immediate and 1 month follow-up radiograph was obtained, and patient’s resolution of clinical symptoms were confirmed (Figure 7). The patient will be monitored for bony healing at 6 months postoperatively.
 Discussion
Discussion
The use of the size XP Finisher to remove the remaining GP on the oval aspects of the root canal wall after removing the main GP core with conventional files and its additional use for activating the irrigant and touching the canal walls to remove the biofilm and place and remove Ca(OH)2 effectively in the canal has been shown scientifically as an effective modality.1-7 The ability to place the sealer accurately while coating the walls completely is also very useful in such cases. Furthermore, the size 30 Finisher acts as great tool for retreatment of hydraulically condensed roots with bioceramic in the oval aspect of the canal. Clinically, the 3D instruments are user-friendly and do not require additional armamentarium for their implementation. The use of the XP 3D Shaper and Finisher to do anatomical shaping through the adaptive alloy technology and their ability to touch root canal walls beyond the reach of conventional files will likely prove to be a welcome addition to conventional and retreatment endodontics. Further research is needed in this area, but the initial clinical experience and outcomes of this technology appear very promising.
[/userloggedin]
[userloggedout][/userloggedout]
 Allen Ali Nasseh, DDS, MMSc, received his dental degree from Northwestern University Dental School in Chicago, Illinois, in 1994 and completed his postdoctoral endodontic training at Harvard School of Dental Medicine in 1997, where he also received a Masters in Medical Sciences (MMSc) degree in the area of bone physiology. He has been a clinical instructor and lecturer in the postdoctoral endodontic program at Harvard School of Dental Medicine since 1997 and the Alumni Editor of Harvard Dental Bulletin. Dr. Nasseh is the President and Chief Executive Officer for the endodontic education company Real World Endo® (RealWorldEndo.com). He is the endodontic advisor to several educational groups and study clubs and is endodontic editor to several peer-reviewed journals and periodicals. He has published numerous articles and lectures extensively nationally and internationally in surgical and nonsurgical endodontic topics. Dr. Nasseh is in solo private practice (MSEndo.com) in downtown Boston, Massachusetts.
Allen Ali Nasseh, DDS, MMSc, received his dental degree from Northwestern University Dental School in Chicago, Illinois, in 1994 and completed his postdoctoral endodontic training at Harvard School of Dental Medicine in 1997, where he also received a Masters in Medical Sciences (MMSc) degree in the area of bone physiology. He has been a clinical instructor and lecturer in the postdoctoral endodontic program at Harvard School of Dental Medicine since 1997 and the Alumni Editor of Harvard Dental Bulletin. Dr. Nasseh is the President and Chief Executive Officer for the endodontic education company Real World Endo® (RealWorldEndo.com). He is the endodontic advisor to several educational groups and study clubs and is endodontic editor to several peer-reviewed journals and periodicals. He has published numerous articles and lectures extensively nationally and internationally in surgical and nonsurgical endodontic topics. Dr. Nasseh is in solo private practice (MSEndo.com) in downtown Boston, Massachusetts.
- Bao P, Shen Y, Lin J, Haapasalo M. In Vitro Efficacy of XP-endo Finisher with 2 Different Protocols on Biofilm Removal from Apical Root Canals. J Endod. 2017;43(2):321-325. Epub 2016 Dec 7.
- Keskin C, Sariyilmaz E, Sariyilmaz Ö. Efficacy of XP-endo Finisher File in Removing Calcium Hydroxide from Simulated Internal Resorption Cavity. J Endod. 2017;43(1):126-130.
- Wigler R, Dvir R, Weisman A1, Matalon S, Kfir A1. Efficacy of XP-endo finisher files in the removal of calcium hydroxide paste from artificial standardized grooves in the apical third of oval root canals. Int Endod J. 2016; Jun 8 [epub ahead of print].
- Alves FR, Marceliano-Alves MF, Sousa JC, Silveira SB, Provenzano JC, Siqueira JF Jr. Removal of Root Canal Filling in Curved Canals Using Either Reciprocation Single- or Rotary Multi-instrument Systems and a Supplementary Step with the XP-Endo Finisher. J Endod. 2016; 42(7):1114-1119.
- Sanabria-Liviac D, Moldauer BI, Garcia-Godoy F, Antonio-Campos A, Casaretto M, Torres-Navarro J, Scalercio JM. Comparison of the XP-Endo Finisher File System and Passive Ultrasonic Irrigation (PUI) on Smear Layer Removal after Root Canal Instrumentation Effectiveness of Two Irrigation Methods on Smear Layer Removal. J Dent Oral Health. 4: 1-7.
- Leoni GB, Versiani MA, Silva-Sousa YT, Bruniera JF, Pécora JD, Sousa-Neto MD. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int Endod J. 2016;Mar 18. DOI:10.1111/iej.12630 [epub ahead of print].
- Azim AA, Aksel H, Zhuang T, Mashtare T, Babu JP, Huang GT. Efficacy of 4 Irrigation Protocols in Killing Bacteria Colonized in Dentinal Tubules Examined by a Novel Confocal Laser Scanning Microscope Analysis. J Endod. 2016; 42(6):928-934.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
