CE Expiration Date:
CEU (Continuing Education Unit): Credit(s)
AGD Code:
Educational aims and objectives
This clinical article aims to discuss the characteristics of files that facilitate cleaning and maintaining the shape of the canal.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions in the CE area to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify some challenges of preventing or eliminating microbes.
- See some characteristics for files that will produce acceptable solutions
- Recognize how different temperature conditions affect the shape of the XP-endo Finisher file.
- Identify the different phases in the process with the XP-endo Finisher file.
Drs. Gilberto Debelian and Martin Trope explain how a finishing file can contact areas that round files cannot while maintaining the original shape of the canal
The challenge
Apical periodontitis is caused by microbes in the root canal, so the practice of endodontics essentially means that microbes should be prevented from entering the root canal in non-infected (vital) teeth or removed when present (necrotic teeth) (Bergenholtz, 1974).
The prevention or elimination of microbes from the root canal poses many challenges. While the vast majority of the microbes are in the main canal and in the planktonic (loose) form, there are complex anatomical irregularities such as accessory or lateral canals and canal isthmuses intercommunicating with the main canals.


In addition, the dentinal walls of the root canal are often covered by biofilm that is particularly difficult to eliminate, as shown by Socransky and Haffajee (2002). While irrigation with disinfectants may be very effective against planktonic microbes, it is not effective enough when the microbes are in the biofilm form or in canal irregularities. In these cases the biofilm must be scraped first before the disinfectant will work. This is analogous to scaling and root planing in periodontal therapy.
The challenge of scraping the biofilm internally in the canal is that almost all canals and roots contain a wider buccolingual dimension compared to the mesiodistal (Figure 1) (Wu, et al., 2000).
Although there are a multitude of file systems with various metallurgical properties and geometric designs available on the market, they all produce a final round shape on any given canal cross section (Figure 2).
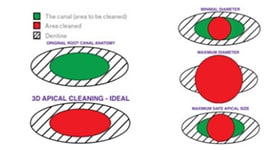
Thus, in root canal instrumentation, the practitioner is limited by the round shape that the file will produce while trying to scrape the walls of the non-round canal and root.
Figure 3 illustrates the limited options for the practitioner because of the disparity of shape between the file and canal/root. The right-hand side represents the options available to the practitioner using round files. The lower left diagram, “3D apical cleaning – ideal” represents the ideal situation, and the upper right, “minimal diameter” is the safest option. The round file fits the narrowest diameter and thus maintains the thickness of the mesiodistal diameter. This is safe but bio-logically unacceptable.
In the “maximum diameter” diagram, the round file is used to the widest diameter. This will remove the biofilm but is, naturally, clinically unacceptable. In the “maximum safe apical size” diagram, the round file is instrumented to the maximum safe apical size, and so while it is not ideal biologically, it is the best we can achieve biologically and if performed correctly is safe for the root. Adjunct methods must then be used to attempt to remove toxins unreachable by the round files.
The “3D apical cleaning – ideal” is the best option, which is to clean the root canal contents only in a three-dimensional fashion without removal of unnecessary dentin.
Recently, the Self-Adjusting File (SAF) (ReDent Nova Ltd., Ra’anana, Israel) has been introduced on to the market (Metzger, et al., 2010) that has, for the first time, shown that it may be possible to clean the widest diameter of the canal without destroying the root structure of the narrow part of the canal. The SAF file requires additional equipment and time and at this point has not been universally adopted by the dental community.
The solution
We feel that the XP-endo Finisher (FKG Dentaire, La Chaux‑de‑Fonds, Switzerland) is the solution after the use of any round file. The finisher has many properties that allow it to gain access and scrape the walls that are untouched when round files are used. In addition, the file causes turbulence of the irrigating solution that also enhances its antimicrobial properties.
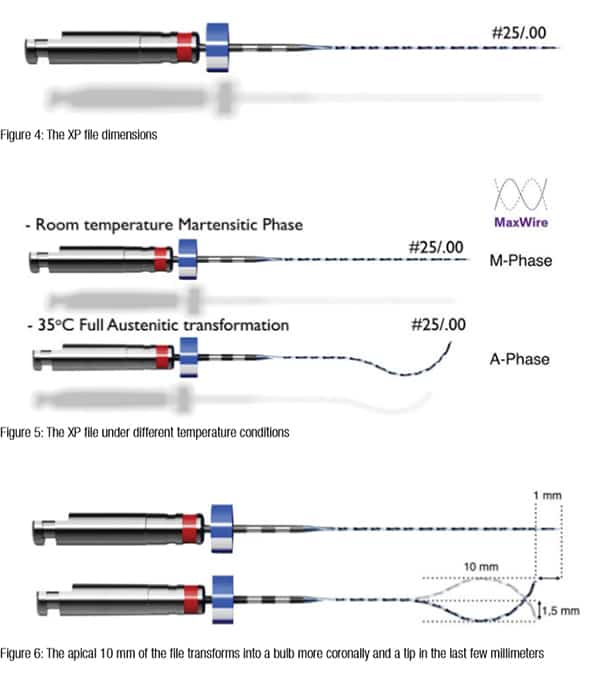
 The file is a No. 25 (.25 tip diameter) with 00 taper (Figure 4). It is, therefore, extremely flexible and thus has tremendous resistance to cyclic fatigue. Its primary action within the root canal is to scrape the walls that it contacts rather than file a (new) shape into the wall of the canal.
The file is a No. 25 (.25 tip diameter) with 00 taper (Figure 4). It is, therefore, extremely flexible and thus has tremendous resistance to cyclic fatigue. Its primary action within the root canal is to scrape the walls that it contacts rather than file a (new) shape into the wall of the canal.
Figure 5 shows the shape of the file under different temperature conditions. When the file is cooled below 35ºC, it is in the martensite phase. In this phase, it is malleable and can be shaped according to the practitioner’s requirements (such as the martensite phase shown in Figure 5). It could also have been bent to any other shape when in this phase. When the file is heated to body temperature (35ºC), it will change to the austenite phase. When the file is rotated in the austenite phase, it creates a very particular cleaning instrument (Figure 6). The apical 10 mm of the file transforms into a bulb shape coronally, while retaining a tip in the last few millimeters. Since the depth of the spoon is 1.5 mm, the total diameter of the bulb and tip is 3 mm. However, if the bulb is “squeezed,” the tip will expand to a maximum of 6 mm; if the tip is “squeezed” the bulb will likewise expand. Therefore, if moved up and down in the canal, the bulb and tip will expand or contract according to the natural three-dimensional diameter of the canal (Figure 7). The maximum loss of length when transforming from straight to full austenite phase is 1 mm. However, it will change to full austenite phase shape in the canal very occasionally.
Importantly, because of the small core diameter of the file, it maintains its flexibility, cyclic fatigue resistance and will scrape, but not shape, the walls. This, plus the turbulence that is created in the irrigant, results in a large surface area of the canal being touched by the file and removes biofilm that would not be removed by round files.
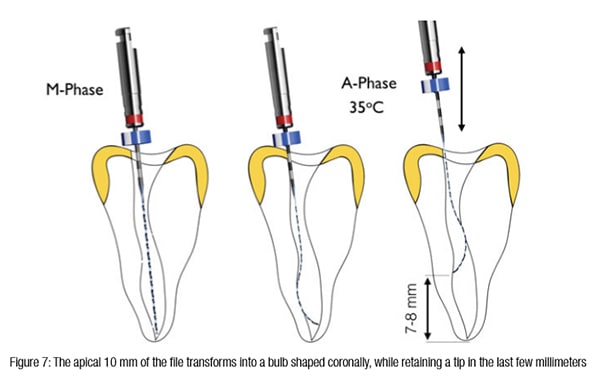
Figure 7 shows the action of the XP-endo Finisher. In the “M-phase” the finisher is placed in the canal before it changes to full austenite phase. The middle illustration demonstrates full austenite phase at canal temperature; the file will expand to the extent that is determined by the canal anatomy. By moving the finisher up and down 7 mm-8 mm, it expands and contracts according to the anatomy of the canal (shown in the right-hand illustration). Thus, the XP-endo finisher has the following advantages:
- It can be an effective adjunct to any file that makes a round shape.
- It is extremely flexible and resistant to cyclic fatigue.
- It molds to the canal shape while not shaping the canal.
- It loosens debris by scraping and agitating the irrigant.
Demonstration and case
Figure 8 illustrates how the finisher will complete the cleaning that is impossible with round files and also maintain the original shape of the canal.


Note that the root has two canals that are irregular in shape in the buccolingual dimension. These irregularities would not be seen in the mesiodistal dimension. The canals have also been instrumented to size 35/04, and in this buccolingual dimension, there is still a large part of the canals that were untouched. In most cases, however, size 35/04 in a root with two canals would look well cleaned.
The XP-endo Finisher is working in the canal. By moving the file in and out of the canal for approximately 7 mm-8 mm, the file tip and bulb will expand and contract and contact all the irregularities in the buccolingual aspect of the canal. In addition, the irrigant is agitated so as to maximize its effectiveness on loosened microbes. Both canals are thoroughly cleaned and additionally, the original shape has been maintained.
Figure 9 is an example of a case where the action of the finisher can be appreciated because the irregularity in the canal is also in the mesiodistal dimension due to internal resorption. The finisher was able to assist in removing debris and tissue in the irregularity, and at the same time, the original shape of the canal was maintained and the root not weakened further.
The preoperative periapical radiograph shows a mesiodistal resorptive defect. The CBCT images show that this is internal resorption and that it extends buccolingually as well. The postoperative radiograph shows that at the second visit, the canal is filled completely, which is an indication that the tissue and debris has been removed. Also, and just as importantly, the original shape of the canal has been maintained so that the tooth has not been further weakened by the cleaning procedure.
Author Info
 Gilberto Debelian, DMD, received his dental degree from the University of Săo Paulo, Brazil in 1987. He completed his specialization in endodontics at the University of Pennsylvania in 1991. He completed his PhD studies at the University of Oslo in 1997. He is an adjunct visiting professor in the postgraduate programs in endodontics at the University of North Carolina at Chapel Hill and the University of Pennsylvania. Dr. Debelian maintains a private specialist endodontics practice in Bekkestua, Norway.
Gilberto Debelian, DMD, received his dental degree from the University of Săo Paulo, Brazil in 1987. He completed his specialization in endodontics at the University of Pennsylvania in 1991. He completed his PhD studies at the University of Oslo in 1997. He is an adjunct visiting professor in the postgraduate programs in endodontics at the University of North Carolina at Chapel Hill and the University of Pennsylvania. Dr. Debelian maintains a private specialist endodontics practice in Bekkestua, Norway.
 Martin Trope, BDS, was born in Johannesburg, South Africa, where he received his dental degree in 1976. He practiced general dentistry and endodontics from 1976 to 1980 and then moved to Philadelphia, Pennsylvania, to specialize in endodontics at the University of Pennsylvania. He became chair of endodontology at the School of Dentistry, Temple University in 1989. Dr Trope is now clinical professor at the Department of Endodontics, School of Dental Medicine, University of Pennsylvania. He is also in private practice in Philadelphia.
Martin Trope, BDS, was born in Johannesburg, South Africa, where he received his dental degree in 1976. He practiced general dentistry and endodontics from 1976 to 1980 and then moved to Philadelphia, Pennsylvania, to specialize in endodontics at the University of Pennsylvania. He became chair of endodontology at the School of Dentistry, Temple University in 1989. Dr Trope is now clinical professor at the Department of Endodontics, School of Dental Medicine, University of Pennsylvania. He is also in private practice in Philadelphia.
References
- Bergenholtz G. Micro-organisms from necrotic pulp of traumatized teeth. Odontol Revy. 1974;25(4):347–358.
- Metzger Z, Teperovich E, Zary R, Cohen R, Hof R. The Self Adjusting File (SAF). Part 1: Respecting the root canal anatomy – a new concept of endodontic files and its implementation. J Endod. 2010;36(4):679–690.
- Socransky SS, Haffajee AD. Dental biofilms: difficult therapeutic targets. Periodontol 2000. 2002;28:12–55.
- Wu MK, R’oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89(6):739–743.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
